Molecular, Cellular and Developmental Biology 3650 — Brain, Thought and Action
Fall 2002
University of Colorado
Riverbend DS Assocation Home Page »
» Term Papers & Reports » Down SyndromeDown Syndrome |
|
Elizabeth Riscoe Molecular, Cellular and Developmental Biology 3650 — Brain, Thought and Action Fall 2002 University of Colorado |
Reproduced with the permission of Prof. Mark Dubin |
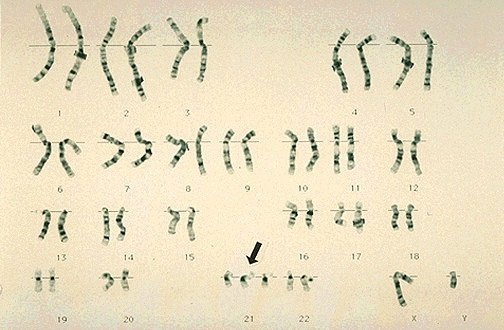
Down syndrome is a chromosomal abnormality which occurs in approximately 1 in every 900 births. The affected individual carries an extra copy of chromosome 21, resulting in trisomy 21. This trisomy is due to nondisjunction occurring randomly during meiosis (gamete formation). The majority of trisomy 21 cases are the result of maternal nondisjunction.
People began classifying Down syndrome as a specific mental handicap about 135 years ago. John Langdon Down, while working as the superintendent of the Earlswood Asylum for Idiots, published the first clinical description of the syndrome. He described patients with similar Asiatic or "Mongolian" features.He attributed these similarities to maternal tuberculosis. However, in 1932, Waardenburg thought the condition was the result of chromosome abnormalities. Lejeune et al. confirmed this hypothesis in 1959 when they found trisomy 21 in 9 infants.
Nondisjunction is the failure of homologous chromosomes (meiosis I) or sister chromatids (meiosis II) to separate and migrate to opposite poles. Due to this, both copies of the chromosome or chromatid go to the same cell. This leaves one daughter cell with 2 copies, and the other daughter cell with no copies of the chromosome or chromatid. When a normal cell fertilizes a cell with 2 copies, the result is a trisomy. Instead, if the cell with no copies of the chromosome is fertilized, the result is a monosomy. Thus, it would be expected that monosomies are as frequent as trisomies. However, monosomic human embryos do not survive gestation, and thus, there are no monosomic births.
Although maternal nondisjunction is the main cause of Down syndrome, nondisjunction can also occur after fertilization. This gives the individual two different cell lines. This is called Mosaic Down syndrome. Some of the person's somatic cells carry an extra copy of chromosome 21, whereas some do not. Typically these individuals do not have as many symptoms as do others with Down syndrome.
Down syndrome can also be the result of a translocation of either the complete or partial chromosome 21.
The characteristics of Down syndrome are due to the individuals' extra copy of chromosome #21. This increased number of genes (found on chromosome 21) is thought lead to increased transcription and translation of these genes, resulting in more of these proteins in individuals with Down syndrome. As a result, individuals with Down syndrome have an altered development.
One critical period of brain development in those with Down syndrome appears to be when the neurons are proliferating, differentiating, and organizing. People with Down syndrome typically show these developmental neuropathologies during this time:
 |
| From Capone (2001) |
Increased oxidative stress is also thought to be related to the development of individuals with Down syndrome.
The oxidative stress that these neurons undergo is thought to influence neuron differentiation and survival.
The increased membrane lipid peroxidation is thought to be critical in the development of neurocognitive impairment over time in individuals with Down syndrome. As discussed below, increased membrane lipid production affects many different aspects of cellular physiology.
 |
| From Capone (2001) |
People living with Down syndrome share many common behavioral phenotypes. Down syndrome is characterized by significant delay in nonverbal cognition, speech, short-term memory and language deficits. These traits are similar to the types of problems others with a mental disability face. However, individuals with Down syndrome are better able to adapt to society than others with a mental disability.
In 1876, Fraser and Mitchell observed the brain of a Down syndrome patient was very narrow in the superior temporal and inferior frontal gyri. They concluded Down syndrome individuals might have problems with speech. This is indeed true. The majority of children with Down syndrome have speech and language abilities which lag behind their nonverbal reasoning abilities. Some general characteristics of this delayed development include:
Adults with Down syndrome show similar speech and language characteristics, many use simple or no grammar. In a study by Rondal and Comblain, it was found that only one-half of the utterances produced were grammatical clauses.
Possible reasons for these speech and language difficulties may include:
Many individuals with Down syndrome overcome these language and speech difficulties quite effectively. They use body language, facial expressions and signals to get their point across when words fail them.
Children with Down syndrome have trouble integrating and processing information sequentially. This links some of their cognitive problems with the short-term memory. The short-term or working memory has been described as 'a mental workplace' because it is essential not only in speech and language, but also for holding and processing information (comprehending what is being read, mental math, or remembering a phone number while dialing it). Possibly the most important part of the short-term memory for those with Down syndrome is the phonological loop.
The phonological loop is the specialized part of the short-term memory which holds verbal information; it holds the sound patterns for words.
When this loop does not work correctly, speech and language will be delayed.
3 ways in which the phonological loop may not function correctly
Reading activities have been found to help improve speech and language difficulties. These activities help to improve the short-term memory of children.
As mentioned above, individuals with Down syndrome are typically better able to interact with those around them than others with mental handicaps. This can be shown through the humor and laughter shown in children with Down syndrome. Humor and laughter can be regarded as only existing in social relations, providing the basis for sociality. Children with Down syndrome were shown to laugh more, and try to entice others to laugh, more so than children with Autism. This helps to show they can reach people on an emotional level, and thus interact more effectively.
Some time or another, we all talk to ourselves. It has been found that adults with Down syndrome often talk out loud to themselves. The Adult Down Syndrome Center reports that 81% of the adults in their study had conversations with themselves or imaginary people. This sometimes leads to concern and can be misinterpreted as a psychological disorder. However, this "self-talk" should not necessarily be a sign for concern.
"You should go with your family, Sam."
"But I want to go to the movies."
"Listen to your Mom!"
"But Sunday is my movie day."
"You can go next Sunday."
Sam ended up attending the family function, with the promise that he could go to the movie next weekend. Whether with himself or an imaginary person, this conversation ("self-talk") helped Sam cope with a situation he didn't like. More about Self-Talk.In children without learning problems, "self-talk" seems to be internalized as the child matures.
"Self-talk" can also be used as a way to express emotions. Their cognitive or speech impairment reduces communication, and therefore, adults with Down syndrome think out loud to process daily events. It can be used as a way to vent anger and frustration.
Individuals with Down syndrome, as human beings, have the right to emotionally satisfying and culturally appropriate sexual expression. As patients, they have the right to routine reproductive health care provided to the general public. However, these rights are sometimes neglected due to societal prejudice and parental anxiety. Parents and caregivers are concerned that the cognitive impairment of Down syndrome makes the individual with Down syndrome more vulnerable to unwanted pregnancy, sexually transmitted diseases and sexual exploitation and abuse. However, when taught the appropriate ways to act in different social and/or sexual situations, individuals with Down syndrome can date and have successful relationships with members of the opposite sex.
The median age at death of individuals with Down syndrome has risen considerably in the last decade, although it still varies between different racial groups. This increase in life span can be attributed to many factors, including: de-institutionalization, better treatments for frequent causes of death, and changes in medical care.
One potential problem with this increased life expectancy is Alzheimer's disease. Alzheimer's disease causes primary progressive dementia. Memory impairment is the standard defining feature, and gets progressively worse as the disease proceeds.
Individuals with Down's syndrome are especially susceptible to this disease due to their extra copy of chromosome 21.
Currently, Alzheimer's disease is diagnosised by the presence of amyloid-ß plaques.
Amyloid ß deposits can be found in most adults (over 30) with Down syndrome. This leads to an obvious increased risk of forming the neuritic amyloid plaques. It has been found that in Down syndrome adults without Alzheimer's disease, the diffuse plaques have formed.
Buckely, Sue. "Reading, Speech, and Language Development."
Buckely, S., Bird, G. "Memory Development for individuals with Down syndrome." (Source)
Capone, G. "Down Syndrome: Advances in Molecular Biology and the Neurosciences." Developmental and Behavioral Pediatrics. 22:40-60.(2001)
Chapman, R., Hesketh, L. "Behavioral Phenotype of Individuals with Down Syndrome." Mental Retardation and Developmental Disablities Research Reviews. 6:84-95 (2000)
Fairbanks, D., Andersen, W. "Genetics." Brooks/Cole Publishing Company. 1999.
Jarrold, C. et al. "Down Syndrome and the Phonological Loop: The Evidence for, and Importance of, a Specific Verbal Short-Term Memory Deficit." Down Syndrome Research and Practice. 6:61-75. (1999)
McGuire, D. et al. "'Self-Talk' in Adults with Down Syndrome." Disability Solutions.
Moore, L. et al. "Reference and Representation in Children with Down Syndrome." Down Syndrome Research and Practice. 5:63-70. (1998)
Reddy, V. et al. "Sharing Laughter: The Humor of Preschool Children with Down Syndrome." Down Syndrome Research and Practice. 7:125-128 (2000)
Reddy, V. et al. "Sharing Humor and Laughter in Autism and Down's Syndrome." British Journal of Psychology. 93:219-242 (2002)
Rondal, J., Comblain, A. "Lanquage in Adults with Down Syndrome." Down Syndrome Research and Practice. 4:3-14 (1996)
Rondal, J. et al. "Down Syndrome: A Review of Current Knowledge." Whurr Publishers Ltd. 1999
Yang, Q. et al. "Mortality Associated with Down's Syndrome in the USA from 1983 to 1997: a population-based study." The Lancet. 359:1019-1025. (2002)