JP DAS Developmental Disabilities Centre
University of Alberta, Edmonton, Alberta, Canada
|
J.P. Das JP DAS Developmental Disabilities Centre University of Alberta, Edmonton, Alberta, Canada |
Reprinted from International Review of Research in Mental Retardation, 26, J.P. Das, Cognitive Aging and Down Syndrome: An Interpretation, 261-306, Copyright © 2003, with permission from Elsevier. |
In 1968, the best known special school in the province of Alberta, Canada, was in Edmonton, founded and run by a nurse named Winnifred Stewart. The school was a model for many in Canada. Its 300 students received no punishment. They were given sensory training, then elementary lessons in the three R's, and life skills and vocational training as they grew into adolescence. Mrs. Stewart had a son with Down syndrome (DS) who was nearing 30 years of age when the author began his research in 1968. Most people "knew" that he would not live beyond the age of 40. Times change. Although Mrs. Stewart was recognized for her dedication and ground-breaking work as the recipient of an honorary doctorate and the Order of Canada, the school was eventually closed. She retired a few years later as the integration and normalization movement spread, although she maintained a keen interest in contemporary research regarding individual differences in cognitive processes, which was being conducted at the University of Alberta's newly established Center for the Study of Mental Retardation. In the ensuing years as the author studied the consequences of aging among people with DS, they began to live much longer. The author even found a few individuals in Edmonton who were over the age of 60 and who are included in one of the studies reported in this chapter.
Some people with mental retardation (MR) are now living as long as those without mental retardation. By the year 2010 the percentage of persons aged 60 and over is expected to increase to 20%, and the number of persons with mental retardation is expected to rise proportionately (Heller, 1997). These figures are of interest to service providers, as is the likelihood that, with increased longevity, many more individuals with mental retardation will develop dementia, leading to both scientific and practical reasons for interest in how people age cognitively. What kind of cognitive processes diminish in the course of aging? Are these the same processes that decline among individuals with DS and" others without DS, but with mental retardation (non-DS)? "The accumulating alarm about premature senescence" and "the uncertainty regarding long-term preservation of function" are in fact worries for individuals with DS (Crocker, 1988, p. 367).
Much has been written about cognitive aging in the "normal" population with erudition and insight (Park & Schwartz, 2000). Although research on the adaptive functions comparing DS with non-DS populations is relatively abundant (see reviews by Heller, 1997; Zigman, Shupf, Zigman, & Silverman, 1993), much less research on DS and the cognitive domain exists at present. The research that does exist frequently follows an eclectic path, testing individuals with and without DS on a variety of tasks without a theoretical thread to bind them. Adopting a theoretical framework for viewing both normal and DS cognitive aging has its obvious liabilities. Such a framework may constrain our inquiry, thus acting as a blinder. This is a cautionary note for adopting theoretically derived measures that differentiate among the three groups of individuals presented in this chapter: "normal," DS, and non-DS with MR populations. Nevertheless, a set of cognitive measures that is derived from a theory is much more interpretable than an eclectic collection of tests and measures. Many share the view that measures in traditional IQ tests do not owe their origin to a theory (for a summary, see Das, 2002). It is not obvious that even the broad components of intellectual abilities, such as adaptive and goal-directed behavior (Sternberg, 1986), have been used as a priori constructs in the making of standardized IQ tests. However, despite the absence of a clear notion of the abilities measured by IQ, researchers have argued about defects versus developmental delays based on IQ that may characterize the population with mental retardation. In recent years, specific abilities, such as memory and attention rather than IQ (or its derivative, mental age), have become the focus of research (Burack, Evans, Klaiman, & Iarocci, 2001). However, in the opinion of the author, the defect versus developmental delay issue did not yield useful results for either teaching or vocational training in Mrs. Stewart's school.
Mrs. Stewart knew that IQ scores did not tell her much about the cognitive processes of her students. When we proposed to study the cognitive processes of three major categories of students (brain damaged, DS, and uncertain etiology) in her school, she was curious to know the results, despite the fact that she had previously refused permission to investigators for a study of IQ at her school. We used tasks that purportedly tested three cognitive processes (discussed later) rather than IQ, which were simultaneous, successive, and planning. Their mean factor scores showed that the DS group was distinctly lower in successive processing tasks compared to the other groups (Snart, O'Grady, & Das, 1982).
The explanation of normal or abnormal behavior can be at many levels. In terms of biology, it is at the level of molecules through synapses, neurons, networks, maps, and systems to the central nervous system (Sejonowski & Churchland, 1989). Within this biological domain, for example, while studying cognitive decline among individuals with and without DS, the upper levels may concern psychologists, whereas the lower levels would interest neurobiologists. Even within the biological domain all the way across molecules to the central nervous system, a defect may be apparent at one level, whereas developmental retardation may appear at another. The explanation at the cognitive level is outside the biological domain, although the scientific aim is to integrate the knowledge of the biological and cognitive domains. Beyond the cognitive domain, explanation at the behavioral domain is still necessary.
A parallel exists in the conceptualization of dyslexia; within this domain of disability, recognition of separate explanations at different levels has become useful. For example, Frith (1999) has suggested that explanations of dyslexia can exist at the three domains of biological, cognitive, and behavioral. Every domain is interactive with environmental determinants. Furthermore, we are reminded that behavioral manifestation is subject to compensatory measures that the individual has adopted to cope with his 01 her disability.
The same schema can be applied to DS and the cognitive consequences of aging. In fact, we may find that for some individuals, their "deficit" has been compensated for in a creative manner. Perhaps a new approach to the old debate on deficit or developmental delay is to be found in Vygotsky:
Vygotsky believed that a child with a defect is not a defective child. A child whose development is obstructed by some deficit—intellectual, sensory, or emotional—is not simply a disabled or retarded child, but has developed differently. The adaptive functions such as overreaching, substituting, equalizing create new detours as it were, for development (Das, 1995, p. 95).
Explanations at many levels in regard to cognitive aging exist but can be integrated to promote theory and research. Li (2002) considered the effect of aging at the three levels comprising biological,-information processing, and behavioral. Data from all three levels are then combined to suggest that the well-known deficiency due to aging in regard to information processing may be determined by deficiencies in neurotransmission. This in turn increases noise and leads to a less distinctive cortical representation, leading to cognitive deficits in such processes as working memory, attention, and speed. In the last part of this chapter, these processes are identified as the major ones in explaining cognitive aging.
Considering cognitive aging and DS/non-DS differences, what is the relevance of the aforementioned discussion? The focus of research by the author and colleagues concerns performance manifested in behavior and cognition, including compensations and the creation of detours, while continually drawing upon biology and genetics. We must remind ourselves that explanation at one level does not diminish the value of explanation at another. However, attempts should be made to integrate them. Second, that the bridge between one domain and another, even bridges between the levels within each domain as described earlier by Sejonowski and Churchland (1989), may not exist. The bridge between biological and behavioral manifestations of Alzheimer's disease and early dementia among individuals with DS, for example, is a case in point. Examples of integrating biological with cognitive sequel of aging are found in research on DS. Schupf (2001) reviewed the neuropathological changes associated with the disease of Alzheimer's type (DAT) in order to understand why DAT symptoms are found frequently in the population with DS above age 50. The reason seems to be as follows: "Before age 50, diffuse plaques are the most common lesion seen in DS, while after age 50, neuritic plaques, containing fibralized <amyloid beta peptides>, predominate" (p. 23). However, how the transformation from diffuse to fibralized results in certain kinds of cognitive deficit and not in others is not clear.
Finally, with regard to DS, non-DS, and normal aging, some cognitive and behavioral expressions are "defective" or "deviant," whereas others are seen as expressions of a "normal" aging process.
In this chapter, the emphasis is mainly on the cognitive explanation with links to behavior. Even when work on brain imaging is discussed in Section IV, the intention is to help understand the cognitive process.
The remainder of this chapter proceeds as follows. First, a model for viewing major cognitive functions, or the planning, attention, simultaneous and successive (PASS) theory, is presented, both to guide the measurement of cognitive function and to unravel the processes underlying performance, which is discussed in later sections. Second, a brief review of cognitive changes due to aging among individuals with and without DS is given. In this review, it would be impossible to avoid references to the connection between DS and Alzheimer's, even though it has been reviewed before and the connection appears well established at present (Zigman et al., 1993). Third, studies on DS and non-DS aging carried out at our own center are discussed. Here we have used both the PASS theory and tests derived from the theory. Incidentally, the tests as currently published (Naglieri & Das, 1997) provide a reliable and age-normed battery of cognitive tasks for individuals with the chronological (thus mental) age of 5 and above. Fourth, a model of normal aging linked to DS aging is proposed and discussed.
The PASS cognitive processing model is described as a modern theory of ability within the information-processing framework. It is based on Luria's (1966, 1970, 1973, 1974, 1980) analyses of brain structures. Luria described human cognitive processes within the framework of three functional units. The function of the first unit is cortical arousal and attention; the second unit codes information using simultaneous and successive processes; and the third unit provides for planning, self-monitoring, and structuring of cognitive activities. Luria's work on the functional aspects of brain structures formed the basis of the PASS model and was used as a blueprint for defining the important components of human intellectual competence. Because thorough reviews of the PASS model and related research are presented elsewhere (Das, Kirby, & Jarman, 1979; Das, Naglieri, & Kirby, 1994; Naglieri & Das, 1990), only a brief summary is provided here.
The cognitive processes that occur within the three functional units are responsible for and involved in all cognitive activity. The first functional unit of attention-arousal is located in the brainstem and reticular activating system (Luria, 1973). This unit provides the brain with the appropriate level of arousal or cortical tone and "directive and selective attention" (p. 273).
Attentional processes are engaged when a multidimensional stimulus array is presented to the subject and the task requires selective attention to one dimension and the inhibition of response to other, often more salient stimuli. Luria (1973) stated that only under optimal conditions of arousal can the more complex forms of attention involving "selective recognition of a particular stimulus and inhibition of responses to irrelevant stimuli" occur (p. 271). Moreover, only when aroused sufficiently and when attention is focused adequately can an individual utilize processes within the second and third functional units.
Luria's description of the second functional unit follows the work of Sechenov. Luria (1986b) described "two basic forms of integrative activity of the cerebral cortex" (p. 74). The processes of the second functional unit are responsible for "receiving, analyzing, and storing information" (Luria, 1973, p. 67) through the use of simultaneous and successive processing. Simultaneous processing is associated with the occipital-parietal areas of the brain (Luria, 1966b). The essential aspect of simultaneous processing is surveyability, i.e., each element is related to every other element. For example, in order to produce a diagram correctly when given the instruction "draw a triangle above a square that is to the left of a circle under a cross," the relationships among the shapes must be comprehended correctly. Successive processing is associated with the frontotemporal areas of the brain and involves the integration of stimuli into a specific serial order where each component is related to the next; i.e., in successive synthesis, "each link integrated into a series can evoke only a particular chain of successive links following each other in serial order" Luria, 1966a, p. 77). In language processing, for example, successive processes are involved as in decoding, production of syntax, and speech articulation.
The third functional unit is located in the prefrontal divisions of the frontal lobes of the brain (Luria, 1980). Luria stated that "the frontal lobes synthesize the information about the outside worlds ... and are the means whereby the behavior of the organism is regulated in conformity with the effect produced by its actions" (p. 263). Planning processes are definitely associated with the frontal lobes. Planning provides for the programming; regulation, and verification of behavior and is responsible for behavior such as asking questions, problem solving, and the capacity for self-monitoring [Luria, 1973). Other activities of the third functional unit include the regulation of voluntary activity, impulse control, and various linguistic skills, such as spontaneous conversation. The third functional unit provides for the most complex aspects of human behavior, including personality and consciousness (Das, 1980).
The frontal lobes of the brain are the last acquisition of the evolutionary process and occupy nearly one-third of the human hemispheres.... They are intimately related to the reticular formation of the brain stem, being densely supplied with ascending and descending fibers.... They have intimate connections with the motor cortex and with the structures of the second block... their structures become mature only during the fourth to fifth year of life, and their development makes a rapid leap during the period which is of decisive significance for the first forms of conscious control of behavior (Luria cited in Sapir & Nitzburg, 1973, p. 118).
Research on the localization of planning has essentially reaffirmed Luria's contention (Das et al., 1994). In a later section, it is argued that older individuals with DS have a core deficit in attention and planning processes.
The PASS theory, shown in Fig. 1, provides a model to conceptualize human intellectual competence that is a blend of neuropsychological, cognitive, and psychometric approaches. Operational definitions of the four processes and the rationale for test construction are derived from the theory (Naglieri & Das, 1990). Consequently, the identification of good measures of each PASS process becomes possible.
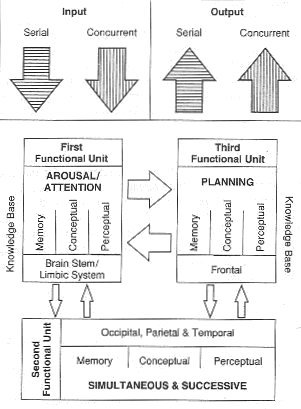
FIG. 1. Planning, attention, simultaneous, and successive (PASS) model. The diagram shows input and output and processing of information. Processing occurs within the constraints of the individual's knowledge base. Note that each of the four processes is broadly associated with one of the anatomical divisions of the brain. Furthermore, each process involves perception, memory, and thinking. From Das, J. P., Naglieri, J. A., Kirby, J. R. (1994). Assessment of cognitive processes: The Pass Theory of Intelligence. Boston: Allyn and Bacon.
As described in Fig. 1, the four components of the PASS model are input, processing, knowledge base (which includes cognitive tools), and output. Each of these has relevance for assessing and understanding the cognitive functions of persons with mental retardation.
Of the four PASS processes, arousal and attention have been studied the most. Visually and auditorially transmitted information are known to evoke elementary forms of attention, such as the orienting response. Given a warning signal and then a target to respond to (i.e., "press when you hear MAN preceded by BOX"), individuals with mental retardation give a greater orienting response to MAN, whereas nondisabled people give a greater response to BOX (Das & Bower, 1971). Arousal and attention are disturbed in hyperactive children, some of whom may also be mentally retarded. Higher forms of attention, as revealed in discrimination learning, have featured prominently as a major limitation of individuals with mental retardation (Zeaman & House, 1963; Krupski, 1977).
In studies of simultaneous and successive information coding, we may find that some individuals have a weakness only in one of these processes and not the other (Das, 1984). In comparing people with brain damage, those with DS, and individuals with mental handicaps without any organic causes, it was observed that people with DS were particularly poor in successive processing. However, individuals with brain damage who also had MR were superior to people with DS and to other individuals with MR in all three processes of planning, simultaneous, and successive processes (Snart, et al., 1982).
Planning or planful behavior is perhaps unique to human beings. Its development is closely associated with the development of language or other symbolic systems, such as sign language, and is represented in the frontal lobes. Planning is one of the most active areas of research in cognitive and neuropsychological functions. People with mental retardation are often thought to be completely unable to plan or to select appropriate strategies. In fact, they are specifically poor in transferring all but simple strategies learned in one situation to another. However, Ferretti and Cavalier (1991) reported a closer scrutiny of problem-solving behavior of people with mental retardation that revealed that some amount of planning and strategy use can be observed in their behavior. The authors suggested that in order to facilitate the transfer of strategies, specific strategy training must be practiced. This suggestion agrees with other observations (Ashman, 1985) that training individuals with mental retardation for the transfer of strategies must be intensive. We would then be able to exploit their limited capacity in planning during problem solving.
The two cognitive activities of working memory and speed of processing have often been related to the deficient general cognitive functions of people with mental retardation. For example, Ferretti and Cavalier (1991) suggested that the slow speed of information processing may be the most critical determinant of poor working memory, which in turn could be the locus of diminished mental ability of individuals with mental retardation. It is more economical to study the PASS components involved in information processing than to study such global components as speed, working memory, and thinking. In other words, speed and working memory deficits can be specifically located in one or more of the PASS tests.
To what extent people with mental retardation may be able to make decisions and judgments will obviously depend on the extent to which they can engage in "planning." Hickson and Khemka (1999) described problem solving and decision making as consisting of the processes that are closer to planning than other processes in PASS theory. It is useful to compare the components they identify that underpin problem solving and decision making with planning components (Das, Kar, & Parrila, 1996). According to them, four processes are identified: framing the problem, generating alternatives, evaluating consequences, and choosing a course of action. Very similar components are identified from the fleuropsychological literature reviewed in Das et al. (1996), which identify goals and objectives as the foundation for planning activities consisting of representation of the problem, anticipation, execution, and monitoring feedback, all of them guided by consciousness. One has to add knowledge base as a prerequisite determinant of all planning and decision-making activities. This is clearly highlighted in practical cases of decision making by people with mental retardation (Hickson & Khemka, 1999).
The knowledge base, of course, is to be assessed as part of any assessment of cognitive functions, including planning. All cognitive processes are based on the knowledge that the person has acquired either formally, through instruction and apprenticeship, or informally, through experience. Informal or experiential knowledge is identified frequently with practical intelligence (Sternberg, 1984). Practical intelligence determines to a great extent the adaptive skills of an individual with mental retardation. Adaptive behavior, apart from living skills, overlaps with social intelligence, including the judgment that the individual displays in social situations (Das, 1984). Judgment itself depends on PASS cognitive processes, especially planning, because of its self-regulatory and self-evaluative dimensions, and on personality factors that include motivation as well. We now know much more about the representation of social intelligence in the brain; the region of the frontal lobe just above the eyes (orbitofrontal rather than dorsolateral part of prefrontal cortex) is currently being investigated as the functional area of different kinds of social intelligence, especially in autism (Frith & Frith, 2001). The relevance of this area is again alluded to in later Section IV while discussing SPECT scan results of individuals with DS.
Cognitive tools are the outgrowth of internal processes and external knowledge, which make human functioning a complex and distinctive activity. These tools include physical entities such as inventions provided by the culture (i.e., computers), as well as the human body itself (i.e., the hands), and less tangible tools such as speech and language that arise out of a child's social interactions. Cognitive tools also include procedural methods of how to solve problems in general (i.e., self-regulation used to approach problems that, for example, require careful completion), as well as formally transmitted knowledge of how to complete a task. It is through the combination of both physical and intellectual tools that higher cognitive activity results (Vygotsky, 1978).
Language is an important tool used for thinking. It is used for planning and mediated learning and, more importantly, plays an important role in the regulation of behavior. In all of these functions, individuals with mental retardation have significant difficulties; this is all the more relevant in case of the limited verbal capacity of individuals with DS. They also experience difficulties using external tools such as computers. Consequently, as an effect of aging, when language use and other cultural tools get harder to use, not only among individuals with, but also those without, mental retardation, cultural learning will be affected adversely.
The last component of PASS that has great relevance for the assessment of mental retardation is output. Many research papers and books have been written on the motor development and deficits in motor development of individuals with mental retardation (i.e., Whiting & Wade, 1986). Simply by providing alternative methods of output, one could enable a person with mental retardation to respond competently. Motor processing strategies can be trained and their development can be recorded reliably, as presented in Whiting and Wade (1986).
PASS is a useful model for the assessment of the cognitive capabilities, including motor development and motor control, of individuals with mental retardation. The model has obvious advantages over assessment of a general intelligence level as obtained from preexisting standardized IQ tests. It has the further advantage of unifying both adaptive and intellectual skills within one theoretical concept. Individual profiles of "special" populations will therefore demonstrate considerable variability in the full range of PASS components, although the total score of the individuals may remain identical. One should regard cognitive aging in special populations as not so special and strange, but as a special case within the general framework of consequences of aging in relation to nonretarded individuals as a group. This will lead to good science and useful practice.
Tests of the four cognitive processes have evolved over a period of 20 years. This research culminated in the Das Naglieri cognitive assessment system (CAS; Naglieri & Das, 1997), which is described in the Appendix. Much of the research with DS/non-DS aging predated CAS using instead an experimental edition of the tests that had high reliabilities and could be grouped into the four PASS processes (Naglieri & Das, 1987). These tests are described in some detail following a brief description of the structure of CAS. Since the availability of CAS, it has been possible to administer a normed and standardized test of cognitive functions in lieu of traditional IQ tests when the objective is to observe individual differences in major cognitive processes. Obviously, normed scores were not available when the four studies (reported later) in our center were carried out. Neither were they necessary in those studies, as the samples of participants contrasted were not compared with the "normal" population. Instead, as described in those studies, the samples comprised adults with mental retardation. They were contrasted on the presence or absence of DS. In future studies, if norm tables for CAS are used, it will be possible to determine the age level (mental age) at which participants are functioning in terms of the four PASS processes.
The following tests are used in cognitive decline. The planning system is the first of four interdependent cognitive systems responsible for "planning," by which we refer to goal setting, strategy selection or construction, and performance monitoring. Planning can be observed in many different forms and at many different levels of task. Examples of planning tasks as well as of other tasks are given in the Appendix.
The attention-arousal system is responsible for maintaining an appropriate degree of alertness in the cortex and for energizing the cortex when needed (e.g., in orienting a response). It is involved in sustained attention (vigilance) as well as in selective attention (when distractors are present). This is a basic function that influences the individual's simultaneous and successive processes as well as planning.
The basic distinction between simultaneous and successive coding is that in successive processing the units of information are connected only by arbitrary, temporal order links, whereas in simultaneous coding the units are related in other, more abstract or quasi-spatial ways (Das, 1973).
Selection from the cognitive tests measuring PASS cognitive processes (CAS) was made from a recent version of the battery described in Naglieri and Das (1987). That article also gives the rationale for constructing the tests from Luria's (1966b) concepts of planning, attention, simultaneous, and successive processes that have been presented and discussed in detail (Das, 1992; Das et al., 1979; Naglieri & Das, 1988). The tests, all of which have high alpha reliability as determined in a try-out version (between .70 and .90), are appropriate for a wide range of mental ages.
Tests from each of the four process measures were chosen for mapping simultaneous and successive processing, planning, and attention. Simultaneous processing was assessed by figure memory (nonverbal) and simultaneous verbal (verbal) tests, whereas successive processing was assessed by color ordering (nonverbal), word recall (verbal), and speech rate (verbal) tests. Attention was assessed by expressive attention (the Stroop tests measuring interference at expressive stage) and receptive attention tests. The planning measures that have verbal and nonverbal items as well were visual search and matching numbers (identifying the two numbers in a row that are identical, the numbers varying from two to seven digits). The details of these tests are provided in several earlier articles (Das & Naglieri, 1992; Naglieri & Das, 1988).
The physical and functional capacities of people with DS decline with age at an accelerated rate as compared to other individuals with and without mental retardation. In addition, there is compelling evidence for a link between DS and DAT (Zigman et al., 1993). DS and DAT have many neuropathological and neurochemical similarities. However, despite the presence of the pathology of DAT, not all individuals with DS develop clinical signs of dementia, although a gradual loss of cognitive function occurs in most individuals with DS. Similarly, DAT is characterized by a progressive decline in cognitive and functional competence, but few studies have documented the changes associated with the course of the illness. Thus DS provides a good model for studying a decline in selected cognitive functions associated both with normal aging and with DAT (Cutler, 1985).
Studies on aging in persons without MR are numerous, but studies involving people with and without DS across the adult life span are rare. Whenever the groups are compared, the object is the onset of DAT. In DAT patients themselves, an assured clinical diagnosis in the living patient has proven difficult. In formulating an operational definition, Benson (1987) included deficits in memory, language, judgment, abstraction, and visual-spatial skills as characteristic of progressive decline in cognitive functioning.
This review conjointly addresses the issue of methodology and the research findings obtained. Although few studies have assessed cognitive decline through the course of DAT, Vitaliano, Breen, Albert, Russo, and Prinz (1984) found that mildly and moderately impaired DAT patients had profiles of memory and attentional deficits that were qualitatively different. Using the dementia rating scale to assess cognitive functioning, Vitaliano, Russo, Breen, Vitiello, and Prinz (1986), in a longitudinal study, found that attention was a powerful measure for distinguishing between mild and moderate DAT groups. Reisberg, Ferns, DeLeon, and Crook (1984) outlined seven clinically differentiable stages in normal aging and progressive dementia, which were further subdivided into five major axes of progressive cognitive decrement. These axes were concentration, recent memory, remote memory, orientation, functioning, and self-care. Reisberg et al. (1984) also examined the utility of psychological test measures in distinguishing early DAT and its various stages. They found that tests such as paired associates, digits forward and backward, and WAIS-vocabulary distinguished between early DAT and normal-aged subjects, but were less valuable in distinguishing early stages from later stages of the illness process.
Another group of studies investigated the relationship between biochemical and cognitive functioning in DAT. Typically these studies (see review by Bowen, Francis, & Palmer, 1987) found a reduction in the activity of acetylcholinesterase (AChE) and a correlation between the clinical assessment of degree of dementia and 4 [14C]-A Ch synthesis. Among the psychometric tests (WAIS, token test, and visual reaction time), only reaction time showed a significant correlation with the rate of ACh synthesis.
Regarding serotonergic neurons, dysfunction was found in the first stage of DAT. Biopsies taken in the first 3.5 years after the onset of symptoms showed that the serotonergic lesion was more severe in the temporal cortex, whereas the frontal cortex was less affected. Other studies found a postmortem reduction in the content of peptides, particularly in the temporal lobe, but it was often spared in the frontal regions. This indicates that there is not a uniformly degenerative process in the neocortex. Other deficits included aphasia and perceptive spatial disorders. Linguistic dysfunction was reflected by low VIQ and token test scores.
The usefulness of PASS tests in detecting dementia is discussed next. Essentially, in the typical procedure, people with and without DS are matched on IQ type tests and then the difference in their cognitive functions is examined using PASS tasks to detect both age-related changes and differences due to etiology. PASS tasks have been used in various experiments on individuals with mental retardation following this procedure (Das, 1972; Das et al., 1979, 1994). Some early variations of the PASS tests for planning, simultaneous, and successive processes were factor analyzed and used to discriminate between individuals with different mental retardation etiologies. A characteristically lower factor score was found for successive processing among people with DS (Snart et al., 1982). These results were investigated further in a later study (Varnhagen, Das, & Varnhagen, 1987), which is discussed in the next section. The tests in this system, however, may not detect all the clinical signs of general dementia. Therefore, a dementia scale and the DS mental status examination form (Haxby, 1989) are recommended as supplements.
In fact, Haxby's study (1989) is especially relevant to the age-related decline segment of the current chapter. He compared 19 young (younger than age 35) and 10 older (older than age 35) adults with DS on some "neuropsychological" tests. His findings from the research carried out within the broader context of relating DS to Alzheimer's (Cutler, 1985) were as follows: Older nondemented individuals with DS were poorer in expressive language than younger individuals with DS. They were also poorer on block tapping (a span test) than on digit span. Older DS participants were worse on a "hidden object" test, which required memory storage for 2 minutes.
The group of researchers at the Institute for Basic Research (e.g., Zigman et al., 1993) has been very productive for some years in delineating the differences and similarities between DS and DAT. It would be redundant to review their work here, but the following sample from the group's recent papers focuses directly on the topic of cognitive processes, rather than on the adaptive behavior of DS, comparing that population to non-DS and Alzheimer cases. The cognitive tests they used in some of their papers were parts of WISC tests, whereas in others, an eclectic battery of tasks was used, similar to Haxby's research cited earlier.
For instance, in a paper (Devenny, Krinsky-McHale, Sersen, & Silverman 2000) using WISC subtests, block design, and coding performance, it was shown that a decline was evident over the observation period in a subgroup of their DS sample. In fact, in cases described as showing "middle stage" dementia, additional subtests from the verbal scale of WISC (vocabulary, similarities, etc.) were sensitive to a decline in intellectual functions. Clear signs of a decline in performance, however, occurred among both DS and non-DS samples beyond age 50.
The question of the reliability of WISC subtests as stand-alone measures of cognitive functions and, more seriously, the nature of cognitive functions that these subtests are purported to measure are unresolved.
Longitudinal studies are sometimes preferable to cross-sectional ones, although the ideal design should contain a combination of both in order to identify the cohort effect and the effect of practice due to repeated testing. With this in mind, results of an earlier study by the same group of researchers (Devenny, Hill, Patxot, Silverman, & Wisniewski, 1992) are worthy of attention. The samples were smaller than the aforementioned study-DS (N=28) aged between 27 and 55 years were compared with a non-DS sample of 18. The eclectic battery of tests included object naming, visuomotor coordination, visual, and auditory memory. Five years of longitudinal testing did not reveal a substantial decline in performance in either of the two samples. An important finding was the absence of a generalized cognitive decline, a fact that supports the findings of our studies discussed in the next section. We do not know why some individuals with DS may not show the .generalized cognitive decline expected at age 50 and beyond, characterizing DAT. Furthermore, a clear picture of the clinical progression of DAT among DS and generally among those with mental retardation is not yet available (Silverman, Zigman, Kim, Krinsky-McHale, & Wisniewski, 1998; Silverman & Wisniewski, 1999). Allowing for the bias of the present author, what adds to the confusion is that the researchers had not used a theory-driven group of cognitive tests in most of the previous studies. Additionally, an overarching model of cognitive consequences of aging as suggested toward the last part of this chapter may help clarify the picture. Anticipating the conclusions of our studies, it would appear that specific cognitive functions framed within a theory of cognitive processes, however, are likely to show a decline.
Due to the eclectic nature of the tests and the small sample size used in most studies, a systematic investigation of cognitive profiles of people with DS as they get to be 40 years and older is still needed. Comparison with non-DS populations is also necessary.
As mentioned earlier, a longitudinal study begun by the Institute of Basic Research (Silverman et al., 1998) is yielding valuable results in regard to DAT and DS. In the studies the author and his colleagues have performed, we have chosen PASS tests defined by a theory and include both DS and non-DS participants. The results have led to a model of cognitive aging with particular reference to DS.
As observed in research by Haxby and others, individuals with DS seem to have a distinct difficulty with language, especially concerning auditory verbal tasks. Older studies, such as a 1967 study by Lenneberg (for a summary see Gibson, 1978), showed that language development was lower in people with DS. More recent work by Silverstein (1982) has narrowed the verbal deficit of DS to difficulties in verbal auditory skills. McDade and Adler (see Varnhagen et al., 1987) indicated that people with DS have deficiencies in processing auditory stimuli and are poor in auditory memory. A verbal auditory deficit can be an indication of a general successive processing deficit, as suggested by Snart et al. (1982). Hartley (1985), supporting the aforementioned results, demonstrated that people with DS were poorer in successive tasks than on simultaneous tasks. Using K-ABC, which has a simultaneous and sequential scale, Pueschel (1987) compared children with DS with their normal siblings and with nonrelated normal children. Children with DS were poor in the two sequential tests: number recall and word order. Both are verbal measures and involve phonological coding. A further examination of auditory and visual processing of verbal stimuli by people with and without DS from our center was performed (Varnhagen et al, 1987). Auditory and visual memory revealed a poor use of the articulatory loop by people with DS, as well as slow long-term memory access for lexical information.
These findings have implications for differential cognitive and neuro-psychological patterns of functioning, which would reflect the progressive deterioration associated with different stages of DAT. Without digressing into the polemics of intellectual assessment, it can be argued that PASS tests, which have a distinct neuropsychological bias, would be sensitive to the differential deficits that would be predictive of DAT stages and would enable a systematic examination of cognitive decline that parallels deterioration in DAT. Such information would be of value to health care practitioners, who are often unable to predict the course of DAT, and may also help family caregivers to cope more effectively with problems that may arise.
Research reviewed earlier illustrates the association between biological and cognitive domains, at times indicating no association. This is not surprising, as bridges between the two domains are often absent. Although we do not yet understand precisely how the two are connected, Zigman and colleagues (1993) presented a strong case in favor of the association between DS aging and Alzheimer's disease. However, the evidence is sometimes only epidemiological, collected from retrospective studies that use autopsy. They point out that differences in research methods can account for anomalies and variations in research results. Even the connection between neuro-pathological changes in the brain of a person with DS (i.e., plaques and tangles) and expressions of dementia behavior are not well understood. "However, at ages associated with extensive neuropathy a substantial proportion of adults with DS do not exhibit clinically significant deterioration in their skills" (Zigman et al., 1993, p. 61). The following statement reflects a consensus: "... a number of studies have shown that the observed increase in risk for dementia is not until approximately 50-60 years of age" (p. 61). Our research also supports the cutoff age to be 50 years, after which cognitive functions decline among DS but not among non-DS samples.
In our research, we have focused mainly on cognition rather than on adaptive behavior, as the latter has been reviewed adequately (Zigman et al., 1993). Heller (1997) also examined adaptive behavior and implications of dementia for caregiving and service provisions in the aging population with mental retardation, which included DS and cerebral palsy.
In the following section, four studies from our center report on (1) use of the dementia rating scale and other general measures of cognitive abilities, (2) factor analyses of cognitive test performance, (3) decline due to aging, and (4) some preliminary results of a study using single positron emission tomography (SPECT).
The first study focused on dementia in individuals with DS across ages from 20 to 65. The major purpose of this study (Das, Mishra, Davidson, & Naglieri, 1995b) was to examine the significant onset of cognitive deficiency among the population with DS. The onset .of dementia was measured by a well-known scale, the dementia rating scale (DRS) of Mattis (1988). The 54 individuals with DS and the 46 individuals without DS but with mental retardation were also examined on the Peabody picture vocabulary test (PPVT), matrix analogies, and the draw-a-person test. We discovered that the DRS shows a significant and sudden decrement when given to DS individuals who are 50 years or older. Down syndrome and non-DS individuals were more or less similar in their DRS performance across the decades from 21 to 50. However, at ages above 50, non-DS individuals did not show a significant drop in their performance in contrast to DS individuals. In addition to this, on each of the five subscales of the DRS, the DS group scored lower than the non-DS individuals at above age 50 as revealed in the significant group by age interaction.
A factor analysis of all the tests given to the DS and non-DS groups taken together is important because perhaps for the first time the results of such a factor analysis are reported in the literature. The principal components, orthogonal solution with varimax rotation, yielded two separate factors that could be simply labeled as verbal and nonverbal intelligence. The first factor had very high loadings on the PPVT and all but one of the five subscales in the DRS, which was the construction subscale, but not the others: attention, initiation and perseveration, conceptualization, and memory. It was a strong factor explaining 58.8% of the variance. In contrast, the second factor explaining only 11.1% of the variance had a high loading on construction and matrix analogies and the draw-a-person, clearly agreeing with the label of nonverbal intelligence. However, in view of the fact that the oblique solution gave more or less the same loadings as the orthogonal solution, we concluded that the strongest factor was verbal intelligence, although some of the tests that loaded on this factor also had significant loadings on this second factor. Of the verbal intelligence tests, the PPVT was useful in that it showed a strong decrement above age 50 for the DS sample.
We also compared DS and non-DS samples on the DRS in relation to published scores for normal elderly and individuals of the Alzheimer's type. Scores of the DS and non-DS samples lie between the normal elderly and the Alzheimer's type groups. This information may be useful for clinicians who wish to detect milder forms of the onset of Alzheimer's. We concluded that the DRS appears to be a good measure of cognitive decline. This conclusion is limited by the small number of elderly DS subjects. The value of DRS in assessing individuals with mental retardation has been investigated further by McDaniel and McLaughlin (2000). They provide "additional descriptive statistics that, along with those provided by Das et al. (1995b), might provide clinicians with reference values when using DRS with clients who have MR" (p. 73). In addition to replicating our results, these investigators "confirm the assertion that the DRS can be administered to most individuals with mild or moderate MR and to some individuals with severe MR" (p. 74). Because these investigators were working on a sample of individuals with MR in the southern United States in contrast to ours in Edmonton, Canada, their research further validates the utility of DRS, based as it is on the objective performance of individuals with MR in contrast to data from subjective ratings obtained from supervisors and caregivers. However, we suggested that for future research it would be interesting to see how specific cognitive processing declines on CAS tasks.
A note about cohort effects is relevant here, as in the aforementioned study, as well as the following ones from our center, comparisons between different age groups are reported. Both in cross-sectional and longitudinal studies, one has to be careful in interpreting decline due to aging (Birren & Schaie, 1977). However, cohort effects are not relevant for the comparison made earlier nor in data presented from subsequent studies in Table III and IV, because in each study comparisons have been made between DS and non-DS samples, essentially demonstrating that whereas cognitive decline in some tests is observed among the first, it is not the case for the second (non-DS). If cohort effects were operating, the comparison between "young" and "old" might show the same trend in both samples. Instead, the studies show an interaction effect between DS/non-DS and young/old.
A factor analysis of planning, attention, simultaneous, and successive processing tasks was taken from an earlier version of the CAS. Two tests from each of these processing scales were selected (see Appendix) and given to the 93 individuals with DS and other etiologies. The results are important in that very often appropriate tests are not found for measuring the cognitive processes of individuals with mental retardation. In this study (Das & Mishra, 1995), we showed first through a principal components analysis, shown in Table I, and later in a confirmatory factor analysis, that three distinct factors could be identified, as shown in Table II.
| Variable | Factor I | Factor II | Factor III |
|---|---|---|---|
| Simultaneous verbal | — | .68 | — |
| Figure memory | — | .74 | — |
| Word series | — | .80 | — |
| Color ordering | — | .72 | — |
| Visual search | .80 | — | — |
| Matching numbers | .85 | — | — |
| Receptive attention | .64 | — | — |
| Number finding | .81 | — | — |
| Expressive attention (Stroop) | — | — | .51 |
| Speech rate | — | — | .85 |
| Percent of variance | 47.7 | 12.5 | 9.0 |
The second one had combined loadings from the two simultaneous and the two successive tasks. We labeled this as a coding factor; as shown in Table I, it explained 12.5% of the variance. The first factor was a combination of attention and planning tasks; it explained 47.7% of the variance. The third factor was distinctly an articulation factor, because the only two tasks that loaded on it required fast articulation: one of these was the Stroop test where color-naming speed was measured and the other was speech rate.
| Variable | Factor I (coding) |
Factor II (attention/planning) |
Factor III (articulation) |
|---|---|---|---|
| Simultaneous verbal | .587 | — | — |
| Figure memory | .705 | — | — |
| Word series | .646 | — | — |
| Color ordering | .837 | — | — |
| Visual search | — | .759 | — |
| Matching numbers | — | .816 | — |
| Receptive attention | — | .722 | — |
| Number finding | — | .845 | — |
| Expressive attention | — | — | .625 |
| Speech rate | — | — | .648 |
| Variable | Group (DS vs non-DS) | Age (25-40 vs > 40) | Group × age |
|---|---|---|---|
| Simultaneous verbal | 4.857b | .139 | .109 |
| Figure memory | 2.058 | 1.510 | .000 |
| Word series | 6.778b | .534 | .128 |
| Color ordering | 2.149 | .012 | .010 |
| Visual search | 3.138 | 1.151 | .054 |
| Matching numbers | 1.860 | .339 | 2.361 |
| Receptive attention | 1.696 | .037 | 3.508 |
| Number finding | 3.009 | .322 | 4.204b |
| Expressive attention | 1.488 | 2.004 | 4.943b |
| Speech rate | 4.434b | 2.414 | 4.568b |
Because three factor scores, representing, respectively, coding, attention plus planning, and articulation, could be obtained from the factor analysis in Table II, we reported an analysis of variance contrasting DS and non-DS individuals in terms of the factor scores. Both coding and articulation discriminated between the DS and the non-DS groups with the non-DS group being superior to the DS group. Contrasted in terms of age, 25 to 40 years in one age level versus above 40 in the other age level, there was no significant difference. The more interesting difference between the groups was obtained in the group by age interaction, which showed a significant deterioration in articulation for the DS group older than 40 contrasted to the non-DS group. The results support the conclusion that individuals with DS may have specific rather than pervasive cognitive impairments at old age relative to the non-DS group. Only 3 of the 10 tasks (number finding, expressive attention, and speech rate) demonstrated a disadvantage for individuals with DS over age 40. A pervasive sensory impairment in the DS group contrasted with the non-DS group due to aging, and therefore, is not supported as the two groups were indistinguishable in the remaining 7 tasks.
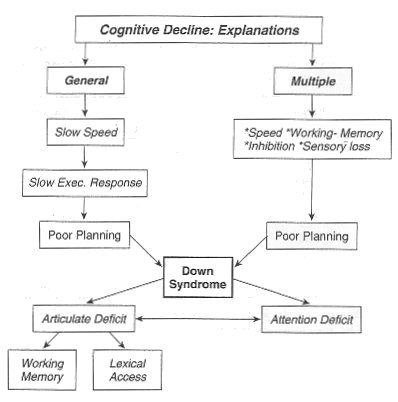
FIG. 2. Explanations of cognitive decline. The top part explains normal aging, leading to the bottom part that provides special explanations for aging in Down syndrome. Cognitive aging among so-called normal individuals, as well as those with DS, is best explained by a multiple processing deficit rather than in terms of one central deficit, which is speed.
Thus, our results show an insignificant contribution by sensory defects, especially dysfunctions attributed to auditory perception, to cognitive decline. The finding is consistent with others, notably that of Marcel and Cohen (1992), in which ah extensive investigation of hearing abilities of adolescents with and without DS was carried out. The only task in which the person with DS performed poorly was in an auditory backward masking task. Thus, hearing difficulties could not predict performance in complex cognitive tasks; rather other information processing mechanisms such as phonological coding (Varnhagen et al., 1987) may be a causal link between auditorily presented tasks and poor performance by individuals with DS. Thus, we suggest that tasks that demand phonological coding and articulation, hence lexical access (see Fig. 2), are likely to show much more sensitivity in the detection of cognitive decline among persons with DS relative to non-DS individuals. However, these results should be checked by a longitudinal study of the aging population with mental retardation. In regard to selecting tests that will be sensitive measures for dementia, we suggest (Fig. 2) the use of those tasks that involve articulation, planning, and attention rather than coding or simultaneous and successive information. We also suggest that early signs of dementia may be detected by those tests that discriminate between individuals with DS and non-DS at age 40 and above.
The main findings, then, of the Das and Mishra (1995) study are displayed in Table IV and were as follows: DS individuals were especially poor in the two verbal tests of information coding and in one test of articulation, irrespective of age, compared to the non-DS group. However, they showed age-related decline even as early as age 40 and subsequently, when older, in three cognitive functions, which were attention, planning, and articulation.
| Variable | Group (DS vs non-DS) | Age (25-40 vs > 40) | Group × age |
|---|---|---|---|
| Coding | 6.792b | .590 | .066 |
| Attention/planning | .792 | 1.205 | 1.793 |
| Articulation | 5.100c | .187 | 3.677c |
In a follow-up study of the DS group 5 years later (see Alexander, 1997), we could still identify 30 individuals who were tested in 1990. Thus, they were retested in 1995. In 1995, they were divided into a young and an old group. The young had a mean age of 32 and the old about 48 years. Their age ranged from 25 to 37 years in the young and 32 to 61 years in the old group. The presence of dementia after 5 years was suspected in the old group. Only planning and attention tasks were administered to these groups, which were followed up after 5 years because previous studies had particularly emphasized the decline in these functions due to age. Specifically two tests, number finding and expressive attention, were found to discriminate between the DS group at age 40 in previous studies. A brief look at the results of the follow-up study again showed that a further decrement had occurred significantly in number finding, receptive attention, and matching numbers. As expected, the older group obviously performed significantly more poorly than the younger group on these tasks. Significant problems in completing some of the CAS tasks in the follow-up group 5 years later were expected and observed. In addition to the CAS tasks, the 30 individuals who were followed longitudinally scored significantly lower on the PPVT 5 years later. Thus, the decline in some of the planning and attention tasks was evident, as well as a decreased performance on the PPVT, which is often used as a verbal IQ test. These results are reported in an unpublished doctoral thesis from our center by Alexander (1997).
A line of research that was begun in our center at the University of Alberta was replicated in a different locale. However, results of that study (Das, Divis, Alexander, Parrila, & Naglieri, 1995a) were quite similar to the previous findings from Edmonton. The study was conducted in Cleveland, Ohio, and examined DS and non-DS individuals above the age of 40, dividing them into younger (40 to 49 years) and older (60 to 69 years) groups. Thus, the chances of finding deterioration after age 40 were increased in this study. The tests given were as follows: the DRS, the PPVT, matrix analogies, and the planning, attention, simultaneous, and successive processing PASS tests.
We found that there was a significant loss of performance in the older group contrasted to the younger one in tasks requiring planning and attention. To elaborate, if planning and attention tasks in this low-functioning population are considered together, it is clear that this component shows the largest signs of cognitive decline due to aging in the DS sample. The DS old group performed significantly more poorly than both young and old non-DS groups in all planning and attention tasks. In contrast, this was not the same for the younger DS group, although its performance was often poorer than that of either of the two non-DS groups. However, it should be kept in mind that our young DS group was actually above 40 years, with a mean age of 44 years. Thus, in comparison with our previous studies, all of them would be categorized as old. Consequently, we suggested that some intellectual decline might have already taken place even in the so-called young group. With regard specifically to articulation deficits, results showed that both groups of DS individuals, i.e., above the age of 40, performed poorly in speech rate and the word series. As expected, the DS group had problems in articulation and auditory processing. This result is consistent with previous findings that language abilities become more impaired than other cognitive processes as people with DS get older. We suggest that poor performance in the speech rate and word recall tasks may be related to difficulties in phonological coding and articulation.
Anticipating the diagram on aging presented in a later section (Fig. 2), it should be mentioned that these performance results should be interpreted with caution, as many of the tests had a floor effect. The DS old group had considerably more trouble in producing correct responses than the other three groups in most of the tests. Thus, while recommending the use of CAS tasks for measuring the intellectual processes of elderly individuals with mental retardation, it is suggested that the tests would work up to as low as 5 years of mental age for which CAS norms are available. In a longitudinal study, however, the number of participants who fail to produce even one correct response in some of the tests due to aging provides usable information in tracing the course of decline in cognitive functions.
In summary, the aforementioned studies from our center show that individuals with DS may have specific rather than pervasive cognitive impairments in old age relative to the non-DS group. Furthermore, because articulation, planning, and attention emerged as distinct markers for age-related declines, it is suggested that these tasks can be used as sensitive measures for dementia.
A study using SPECT was carried out in our center on 11 DS individuals between ages 33 and 61 years as reported in Alexander's (1997) dissertation. SPECT requires the procedure of injecting a radiopharmaceutical agent. Results are shown in a series of multicolored images reflecting regional differences in perfusion, an index of metabolism in the brain. Thus, the SPECT scan is expected to show the status of cerebral blood flow. More specifically, as the following reviews on SPECT suggest, a bilateral decreased cerebral blood flow in the temporal-parietal region is likely to be observed (Schapiro, 1993).
In addition to Shapiro's research and review, only a few other important research articles are worth mentioning here. In research reported by Maruyama, Ikeda, and Yanagisawa (1995), 17- to 55-year-old DS individuals were scanned with SPECT. Of the 11 patients with DS, 9 patients had been found to have DAT. In a study by Gokcora (1999), a sample of 17 young individuals with DS between ages 3 and 24 with a mean age of 10.9 years participated in the research. None of the patients, of course, had dementia symptoms. Brain perfusion scans using SPECT were analyzed visually. Nine out of the 17 DS individuals showed normal brain perfusion, whereas the remaining 8 revealed hypoperfusions that were not typical of Alzheimer's disease: the hypoperfusions were mostly unilateral rather than affecting both the right and the left halves of the brain. It was also spread over parietal, temporal, occipital, and frontal areas. This side-to-side asymmetry and unilaterality are not considered typical patterns of dementia related to Alzheimer's type perfusion deficits found in DS. However, the study is of limited value for the present topic on aging except to establish that the SPECT procedure can be applied meaningfully to the very young and to offer a contrast between young and old.
As reviewed earlier, the development of dementia is marked by a symmetrical bilateral blood flow reduction rather than an asymmetrical one affecting only one half of the brain (Mori & Nakata, 1993). However, an asymmetrical hypoperfusion may be a precursor and a warning for the possibility of developing DAT. This seems to emerge as a general conclusion with few exceptions. Even in younger DS cases aged 30 to 8 years, Kao et al. (1993) observed a significant unilateral (hence asymmetrical) reduction in blood flow in the temporal-parietal-occipital region when they did SPECT scanning on 14 DS individuals, forewarning the possible onset of DAT. DAT was distinguished from other dementias: reduced cerebral blood flow to the parietal-temporal cortex and not involving other regions such as the sensory motor cortex, basal ganglia, occipital region, or cerebellum.
In our work, 11 participants (7 males), between the ages of 33 and 62 years, with a mean age of 48, were studied.¹ Written informed consent was obtained from each participant and his or her guardian. Each was also asked before taking the injection if he/she wanted to participate. A few withdrew.
Each participant was injected with between 70 and 1000 MBQ (routine dose), 99mTc HMPAO through a line inserted in the anticubital fossa. During injection, each participant completed an easy visual search task (searching for a picture embedded in a field of numbers). Following injection, a rapid sequence of images was obtained on a gamma camera/ computer system to assess arrival of the radiopharmaceutical. On completion of the imaging, the participant was free to leave, as there are no residual side effects of the procedure.
The SPECT scan was expected to show a bilateral decreased cerebral blood flow in the temporo-parietal region. All of the 11 consenting DS adults showed "abnormal" SPECT scans compared to the records of the cancer institute where the scanning was carried out. Specifically, 7 of the 11 cases clearly showed Alzheimer-like changes: reduced temporal lobe perfusion was observed (Schapiro, 1993).
SPECT has been used recently to differentiate between DAT and fronto-temporal dementia (Waltz, Knowlton, Holyoak, Boone, Mishkin, de Menezes Santos, Thomas, & Miller, 1999). The objective in that report was to relate reasoning ability to damage to a specific region of the prefrontal cortex. Studies such as Waltz et al. (1999) and Alexander's (1997) open up the possibility for pinpointing the damage by means of SPECT and other neuroimaging techniques and then using individual differences in the DS performance on tests such as CAS to correlate regional variations in the metabolic activity of the brain.
Why do some older individuals do poorly in tests of intellectual ability, including IQ tests? Although an age-related decrement in IQ has been suspected for a long time, perhaps since 1920 (Deary, MacLennan, & Starr, 1998), little explanation has been given. Perhaps the best way to begin answering this question is to pose different questions: What are these tests measuring and what cognitive processes may underlie their assessment of the aged?
Faced with the enormity of performances, skills, and strategies that fall under the umbrella of "cognitive functions," it would be an oversimplification to attribute the general decline of cognitive function to a single variable. Similarly, considering the number of cognitive operations attributed to different regions of the brain that contribute to even a single cognitive function, neither can we easily isolate the factors responsible for decline of a specific cognitive function. In fact, the literature on age-related cognitive decline shows a variety of factors contributing to age-related deficits across a number of measures, with varying degrees of correlation (Birren & Schaie, 1977). In general, we can divide the proposed explanations for decline into two categories: resource deficit and resource allocation. That is, we can ask to what extent is age-related decline among older adults due to a decrease in cognitive resources such as processing speed, recall, and working memory? What is due to the less efficient use of resources by the individual, explained through an age-related decline of inhibitory mechanism, effort, attention, and planning ability?
On a higher causal level, research in this area suggests that the strong connection found between sensory and cognitive functioning may actually be indicative of a general decline in central nervous system function (Baltes & Lindenberger, 1997; Lindenberger & Baltes, 1994). However, single cause hypotheses may not be able to explain the increased variability between older subjects on such measures as reaction time, memory, and fluid intelligence as compared to a younger cohort (Morse, 1993). Pending further examination, results of many studies suggest that not one, but several relatively independent age-related factors are responsible for cognitive decline. This hypothesis is reiterated and supported substantially by research into task-specific slowing, where a greater age-related decline is shown on tasks relying primarily on speed rather than knowledge (Kliegl, Mayr, & Krampe, 1994; Kaufman & Horn, 1996), as opposed to generalized cognitive slowing.
The model, which presents an overview of contemporary explanations of aging, is presented in Fig. 2. The model is explained part by part. The top part of Fig. 2 relates to "normal aging" and the bottom part to special characteristics of aging among the DS population. Based on our research and the findings of many other researchers, we suggest that for explaining cognitive aging among individuals with mental retardation, two cognitive components can be identified for special emphasis: articulation deficit and attention deficit. These, however, overlap with multiple processing decline explanations. Clearly, a general decline of all cognitive processes is not favored as an explanation for either normal or DS aging. The subsequent sections deal briefly with the main cognitive components of Fig. 2.
Many relatively independent age-related factors are responsible for cognitive decline. However, in the literature of the resource-deficit explanation of cognitive decline, the simplest explanation for an age-related decline in speed-dependent tasks is a decline of processing speed. Reductions in speed and accuracy on test performance indicate that the deterioration in both appears to be mediated by a slower rate of executing cognitive functions, which is part of planning (Salthouse, 1994, 1995).
Another causal chain of decreased cognitive functioning suggests that age-related reductions in processing speed mediate age differences in working memory, which then mediate differences in feedback usage. This in turn influences planning (executive functions). A popular measure preexisting in the tests within the PASS framework is the Wisconsin card sorting test (Fristoe, Salthouse, & Woodard, 1997). However, such an apparent linearity of cause does not fully account for the entire variance across cognitive domains. Research obtained by testing subjects with the Wisconsin card sorting test (cognitive performance), the Benton facial recognition test (cognitive performance), the P300 latency of auditory-evoked potential (processing speed), and standard measures of cardiovascular health did not support either processing speed or cardiovascular health as single causal factors of age-related cognitive decline (Dywan, Segalowitz, & Unsal, 1992). In any case, as PASS theory will suggest, the cognitive process of planning is at a higher level than processing speed. Thus, it is important to recognize the plans and strategies that are used while an individual may be solving a problem or executing a task speedily.
Speed is not of one kind. It has at least two different connotations that must lead to very different explanations of decline in cognitive performance. These are "speediness" and "speed" (Nettelbeck, 1994). Speediness is conceived as quickness in test performance when the test is undemanding and overlearned. This is an operational definition without hidden theoretical connotations. Speed, however, has come to be more popularly accepted as the speed of information processing as measured by reaction time. Claims have been made that it is the measure of central nervous system efficiency; however, this is questionable. Although it may be attractive to believe that speed is a reflection of biological and culture-free intelligence, even a slight delving into the biological domain (from molecules to the central nervous system) appears to make this concept untenable. If synaptic activity means the speed of release of appropriate neurotransmitters, how does one consider speed of inhibition that slows down and even eliminates a neural response?
At cognitive and psychometric levels, it is not clear what the construct of "speed" in tests such as reaction time and inspection time measures exactly. As Nettelbeck (1994) suggested following Horn, when elderly persons show a slowing response time, this "may reflect executive capacities controlling concentration rather than speediness" (p. 1017). This is in line with the model of cognitive decline (Fig. 2) in which attention is an important cognitive deficit that characterizes the elderly person with DS. The construct of speed as operationalized in various other tests of information processing does not yield a unitary factor either. The speed of reading simple words and naming colors, for example, loads on a separate factor from speed of visual search and trail making (joining numbers from 1 to 25 scattered on a page in serial order) as shown by Das and Dash (1983). A decrement in general speed of activity in old age is so common that scientific research does not have to prove it. In conclusion, as was suggested previously, it is best to conceptualize speed specifically in terms of distinct cognitive processes such as speed in planning and executing a response and in allocating attention. In sum, as suggested in Fig. 2, elderly persons, including those with DS, are slow in response time because they may be poor in executive capacities controlling concentration and attention. The DS population has additional difficulties in attentional processing. The role of failure in planning in cognitive decline is elaborated in a subsequent section.
A consensual definition of "working memory," a term coined by Baddeley and Hitch (1974), is as follows: "Working memory is the system (or more accurately, the set of systems) responsible for the temporary storage of information during the performance of cognitive tasks" (p. 21). The concept includes the phonological loop, a visual-spatial "scratch pad," and a central processor. It is one of the four factors that account for cognitive decline in old age. Although placed within the context of multiple explanations rather than a single general explanation of cognitive loss, the concept could be associated with general deficiency if it is viewed, as suggested by Park and Schwartz (2000), as the total amount of mental energy available to perform online mental operations.
The precise relationship between working memory and aging is not established simply because the explanation for cognitive decline can be found in some or all of the component processes associated with the concept. Examples include a decline in self-initiated processing, a diminished ability to process auditorially presented items, rehearsal failure, poor phonological representation, and obvious poor central processing. This last example can be linked readily to planning or executive processes. Thus, although apparent working memory failure can be described as a resource deficit, its deficiency is associated with the central processing component as a resource allocation deficiency as well.
Memory for sequence is a successive process. In specific reference to DS, working memory deficits must be considered within the broader context of mental retardation. Typically in a test of working memory (interchangeable with memory span), we are testing immediate recall of the serial order in which items are presented. Two different processes influence memory for order: first, the item such as the name of the digit, letter, or word must be encoded. This requires consulting the appropriate lexicon in the head, as it were. The longer it takes to find the right name for the item, the worse will be the individual's performance on recall tasks. For the individual with mental retardation, this time is longer than for normal nonretarded individuals. A significant allocation of attentional resources for encoding the items is required for producing a name for the digit or letter and to recognize and read a word. This exists mainly due to poor lexical access. The second influential determinant is successive processing. Individuals with, compared to those without, DS can be significantly behind in both (Das, 1985). DS aging can diminish encoding efficiency and successive processing abilities. A related component of working memory is rehearsal, which is influenced by the speech rate. Thus an explanation in terms of slow or defective speech among individuals with DS may be used as an explanation. However, research by Jarrold, Baddeley, and Hewes (2000) has ruled out the idea that DS participants are lagging behind in rehearsal; therefore, their obviously slow speech rate may not be the explanation for their poor memory span. This finding leaves open the two processes of (1) slowness or deficits in encoding and (2) poor successive processing as possible explanations. The discussion on working memory applies to short-term memory (STM) research findings as well.
The implications of all these theoretical explanations for intervention and retraining are important. For people with DS, rehearsal training is not recommended for improving working memory. The other recommendation is to avoid the requirement of speech output as a condition for recall tasks. Persons with DS, in contrast to those without DS, have well-known problems in producing oral speech (articulation deficit). Rather, better training in phonological encoding "and successive processing, together with measures to improve attention, will be effective.
Older adults show an age-related decline in the ability to suppress goal-irrelevant and distracting information (Carlson, Hasher, Connelly, & Zacks, 1995). This is explained in terms of an age-related decline in inhibitory mechanism (Hasher & Zacks, 1988) and accounts for a reduced efficiency of working memory with age. Due to a decline in inhibition, working memory gets cluttered with irrelevant information, resulting in distraction. Lack of attention is a problem with older people, especially for those with DS. It must be apparent from the aforementioned discussion of explanations for cognitive decline that each of the determinants-working memory, speed, and inhibition-can be identified as the single most important cause of cognitive aging. Each has been identified to define "intelligence." In summary, with special reference to DS, it can be concluded that inhibition loss directly explains cognitive aging among this population, mainly by causing attention deficit. For example, inhibition failure diminishes selective capacity, which in turn results in the individual's inability to prevent irrelevant information from gaining attention. The nature of inhibition itself ought to be understood in relation to attention. The components of working memory, inhibition, and attention are interdependent rather than independent in the model proposed in Fig. 2.
Another general statement relating to Fig. 2 concerns the role of knowledge base. All cognitive processing is integrated with knowledge base; this has been emphasized in the PASS theory. Apart from an efficient retrieval of knowledge, older people are hampered by a lack of growth of knowledge. Acquisition of facts and skills are slower in old age. This author suggests that the weakness permeates all mental functions, but particularly diminishes the ability to plan and make decisions. Programs for intervention or cognitive enhancement should, then, focus on reinforcing both acquisition of new knowledge and strategies for retrieval of knowledge.
Perhaps the unifying disability in old age is a gradual loss of sensory functions. As discussed by Park (2000), the Berlin aging study by Baltes and Lindenberger suggested that sensory measures continue to decline from age 25 onward. "Sensory measures provide an index of neuronal integrity which in turn mediates cognitive function" (Park & Schwartz, 2000). What is its implication for intervention? In regard to the DS population, a sensory defect in hearing and a motor deficiency in speech production mechanisms are common. The weaker sensory measures are likely to deteriorate earlier. These should be relevant in designing rehabilitation programs for the aging DS population.
Explanations for cognitive decline converge on planning as shown in Fig. 2. Planning comprises programming, regulation, and verification of behavior (Luria, 1966). An individual adopts a set of decisions and strategies and modifies them while solving a problem and reaching a goal. This is planning: the essence of intelligent behavior. Within the context of intelligence as a sum total of all cognitive processes that include planning, attention-arousal, simultaneous, and successive processes, planning occupies the highest status (Das et al., 1994). Planning processes are closely connected with attention on the one hand and with simultaneous and successive processing on the other. In assessing an individual's information processing skills, planning processes are needed when a test requires that the individual make decisions about how to solve a problem, execute an approach, activate simultaneous and successive processes, monitor the effectiveness of the approach, and modify the approach as needed. We have also argued that planning can be a more pervasive regulatory process than problem solving. It is oriented toward the future and may include the creation and selection of problems, as well as the anticipation of a sequence of actions to solve them. Instead of being a hierarchical and linear process, planning is often nonlinear and revisionary in nature, and the formation and execution of a plan can occur simultaneously. Planning is a self-organizing, reflective process of which the individual is conscious, at least at some point of its development, and requires motivation and metacognitive skills. It is an activity that integrates several different components and levels of functioning into one schema and is a uniquely human function with close connections to speech and language (Das et al., 1996).
Is planning or executive function a resource deficit, like speed, that suffers decay in old age? Alternatively, should we consider it as a problem of resource allocation related to aging? It can certainly belong to both categories. Elements of planning include representing the problem at hand, anticipation, execution, and monitoring feedback. DS and non-DS differences are not particularly apparent in planning or executive functions. Instead, we find the DS population specially characterized by articulation and attention deficits compared to non-DS populations.
The aforementioned model of aging (a) links general cognitive consequences of aging to aging in people with mental retardation and (b) highlights the characteristics specially observed in people with DS. Thus, it is an attempt at building an abiding model supported by research as discussed earlier, although requiring further thought.
In conclusion, the major concepts that are interwoven throughout the chapter are presented.
We have had a hundred or more years of general intelligence or "g." The research on multiple components in cognitive aging has moved aside, if not destroyed, the relevance of "g". Even the new incarnation of "g" as "speed" is challenged as a sign of overall intelligence simply because knowledge base and the specific cognitive processes such as those in PASS cannot be ignored or explained by "speed", as "g". Luria's original proposal for functional organization, as operationalized in PASS theory, is much more useful. As shown in this chapter, the core ideas of Luria are still relevant in understanding cognitive differences in aging. However, PASS tests and specifically tests included in the Das-Naglieri cognitive assessment system may be too difficult for some participants among old DS and non-DS individuals. Alternative tasks within the PASS context are needed for those cases.
The PASS theory has evolved and can accommodate the core concepts in aging such as speed, working memory, and inhibition as discussed in the "binding model." New advances in neuropsychology guide continuous revisions of any model of mental processing and PASS is no exception. An attempt at understanding Down syndrome in terms of a decline in planning due to difficulties in language is a new direction for research (Das, 2002). If the planning deficit is linked with a deficit in phonological memory and language deficit, then it becomes important to know how exactly language is used in planning, not only among individuals with DS, but also in other groups such as those with hearing loss. The important role neuroimaging techniques will play in investigations such as this is alluded to next.
Dementia in DS may differ from DAT, which is mainly characterized by memory loss. The aging model described in this chapter supports that argument. The contrast between DS and DAT may decrease with age, especially after age 50. As the DS/non-DS comparisons demonstrate in the studies from many research centers, including ours, specific differences between the two groups in cognitive and SPECT measures are noticed. The cognitive profiles of people with and without DS differ even before aging is entered as a variable. Individuals with DS, as expected from earlier research, are relatively weaker in verbal coding and articulation. A deficit in lexical access is suggested as a core problem in the "binding model." As a consequence, among those with DS, successive processing is found to be characteristically poor. This has little to do with their auditory processing. As the individuals with DS grow older, further specific deficiencies may be observed in attention, planning, and articulation. Help from neuroimaging techniques is fortunately available to study the damage to cognitive processing. Although relatively few studies that focus on the DS population currently exist, their results are surprisingly clear. Using SPECT, a less expensive technique compared to positron emission tomography (PET), many of the aging DS individuals typically show a reduced blood flow to the temporo-parietal regions of both the left and the right halves of the brain. However, much variability exists as the SPECT data presented in this chapter showed. The importance of treating each elderly individual with DS as a unique case cannot be overemphasized. Future research may answer many questions in regard to SPECT and PET scanning of DS and non-DS brain activities during test taking, rather than after a test has been administered for a very brief time, as was done in our SPECT experiment. Is there a developmental change from unilateral to bilateral in the pattern of reduced blood flow (hypoperfusion)? In what percentage of older adults do cognitive dysfunctions coexist and can be correlated with hypoperfusion in specific brain areas? For example, can we speculate that the low metabolism in the temporo-parietal region coincides with the typically limited capacity of the older DS individuals for phonological processing (hence working memory) and attention? The SPECT study that was reported did not use scanning when the participant was engaged actively in doing one of the successive or attention tasks, and hence one could not connect the images to activity during task administration. Comparison between people with and without DS under such conditions will contribute spectacularly to our understanding of aging and its cognitive consequences in individual cases. Perhaps until then, the explanation of cognitive decline proposed may remain as a reasonable hypothesis to be worked out further and ultimately tested by direct correlates of brain functioning.
How have the explanations at all three levels helped research and practice in regard to Down syndrome and aging? This entire chapter has much evidence in supporting that these multilevel approaches are quite appropriate, although we are still searching for bridges to cross over from one level to another. To start with, the PASS theory is an example of the integration of cognitive and neuropsychology as it stretches back to the classical work of Sechenov, followed by Luria's functional organization of the brain. Information processing is the central concept in both cognitive psychology and neuropsychology, as also in the recent research on aging reported by Li (2002). Such cross-level theorizing by Li attempts to link a reduction in catecholaminergic modulation, neural network modeling, and a basic property of information processing, which is a noise-to-signal ratio on the one hand and such broad cognitive functions as speed and working memory deficits due to aging on the other. Many bridges are crossed in this research, many more than the SPECT scan research reported in Section IV. Switching to explanations at the cognitive level, the tentative model presented in Fig. 2 summarizes most of the available knowledge in cognitive aging and extends it to Down syndrome. Each of the cognitive constructs needs further research within the context of aging specific to Down syndrome, as well as in regard to other special populations, such as those who suffer from language deficit due to hearing loss. The idea here is to study a central cognitive concept, language use in planning process, across different populations, including "normals." Such cross-population research can then enrich our knowledge of cognitive processes.
Finally, what practical implications does the research reported from our center have for managing the behavior of individuals with DS who are living longer? Individuals with mental retardation with moderate cognitive dysfunction at age 40 and older need extra assistance in reducing the stress on attention and planning. This recommendation is consistent with conceptualization that aging affects these cognitive processes adversely (see Fig. 2). One method is to remind the individuals often about the relevant aspects of the working environment that need attention rather than assuming that they are always alert and reliable workers. An important problem relates to drowsiness and catnaps, as well as to the general problem of maintaining their interest in their work. Because of a low state of arousal, any slight increase in task demands may make the individual irritable, which can be misconstrued as a behavior problem among older individuals.
A reduced demand on planning daily routines and chores at home as well as in the workplace is essentially required for aging (over 40) individuals with DS. Disturbing a routine of activities and changes in living arrangements are just two examples of events that require new planning; the individuals need a great deal of assistance in learning again to plan their activities.
There is a distinct disability found in individuals with DS that relates to articulation. Persons with DS are likely to suffer an impairment in articulation (Fig. 2)—expressing themselves quickly and fluently. Their speech may be slow. Patience is required on the part of supervisory staff when they are expecting a verbal answer from the individual with DS. Persons with DS may not be able to express their physical needs intelligibly. They may not be able to communicate their feelings (likes and dislikes, depression and anxiety) clearly. They may not be able to repeat the instruction of the supervisor to show that they understand it, yet their understanding may be good. Therefore, especially in the case of individuals with DS, speech may appear to be bizarre because of their inability to suppress irrelevant speech and to express selectively what they wish to say at the right place and time. Thus, in addition to difficulties in attention and planning, persons with DS are especially handicapped in expressing themselves fluently and give the impression of being incoherent. These are some examples for improving the adaptive behavior of the aging population considered in this chapter.
In retrospect, if there is a central message that emerges from the work reported in this chapter, it seems to be the one suggested by Luria: Between the mind and the body, there is no duality (Das, 1994).
The CAS is an individually administered test designed for children and adolescents aged 5 through 17 years. The tests consist of 12 regularly administered subtests, which are organized into four PASS scales. There is also a total score called a full scale (FS). PASS scales and FS standard scores can be obtained using two combinations of subtests. One combination is called the basic battery and the other is called the standard battery. The basic battery includes 8 subtests (two per PASS scale); the standard battery includes all 12 subtests.
The full scale score is an overall measure of cognitive functioning, with a mean (M) set at 100 and a standard deviation (SD) set at 15. The score yields a measure of the child's overall level of cognitive functioning based on the four PASS scales.
PASS scale scores (each with a M of 100 and a SD of 15) are composed of the sum of subtest scaled scores included in each respective scale. These scores represent a child's cognitive functioning in specific areas and are used to identify specific strengths and weaknesses in cognitive processing. PASS scales, not PASS subtests, are the focus of CAS interpretation.
Subtests (each set at a M of 10 and a SD of 3) are measures of the specific PASS process corresponding to the scale on which they are found. They are not considered to represent their own set of specific abilities, but rather are measures of one of the four types of processes. They do vary in content (some are verbal, some are not; some involve memory, others do not, etc.), but the most important point is that each is an effective measure of a specific PASS process.
The CAS was standardized for children aged 5-17 years using a stratified random sampling plan that resulted in a sample that closely matches the U.S. population. Children from both regular education and special education settings were included. During the standardization and validity study data collection program, the CAS was administered to a total of 3072 children. Of that sample, 2200 children made up the normative sample, and an additional 872 children participated in reliability and validity studies. A group of achievement tests was also administered to a 1600-person subsample of the 2200-person standardization group.
The CAS standardization sample was stratified on the basis of age (5 years 0 months through 17 years 11 months), gender (female, male), race (Black, White, Asian, Native American, other), Hispanic origin (Hispanic, non-Hispanic), community setting (urban/suburban, rural), classroom placement (full-time regular classroom, part-time special education resource, full-time self-contained special education), educational classification (learning disability, speech/language impairment, social-emotional disability, mental retardation, giftedness, and nonspecial education), and parental educational attainment level (less than high school degree, high school graduate or equivalent, some college or technical school, 4 or more years of college). Methods used to collect data were designed to yield high-quality data on a sample that does closely represent the U.S. population; for details on the representativeness of the sample, see Naglieri and Das (1997).
This task is similar to that developed by Teuber, Battersby, and Bender and found by Ashman and Das (1980) and Naglieri and Das (1988) to load on a planning factor. The subject was instructed to point to a picture, number, or letter located in a field around the target, which appears in a stimulus box. Each item included two searches per page, one located on the top and the other on the bottom of an 8.5x11 inch page. Items were timed from the point of exposure to the moment the second target was found. The total score was the sum of all 20 items. Search tasks consisted of digit targets embedded in randomly organized fields of digits, letters among letters, and pictures among pictures.
This task is associated with the planning factor in previous research (Naglieri & Das, 1988). The task required the subject to find and circle two numbers that are the same on each of eight rows per page. There were six numbers of the same length per row. The numbers increased in length from one to seven digits over the three pages of items. The score was the number correct within the time limit for pages 1-2 (grades K-2) and 1-3 (grades 5-12).
This task is composed of two pages containing rows of picture pairs. On the first page the subject circled, row by row, all the pairs of pictures that were physically the same (i.e., two pictures of a house, but not a house and a bird). The second condition was similar, except that the subject circled all of the pairs of pictures that had the same name (i.e., two different houses or birds, but not one house and one bird). The test contained pictures of a bird, face, tree, flower, and fruit. In the first condition, identical pictures were targets, whereas in the second condition, pictures from the same category were targets.
This test is a self-paced, vigilance-type task. The subjects were given a printed sheet of single digits from 1 to 9; 9 digits per row are arranged randomly. In the form of the test that was used for subjects with and without DS, subjects are asked to cancel selected digits when they come across digits 1, 2, or 3. There are 18 rows of digits.
This test is similar to the Stroop test. The version we used defined an attentional factor (Das, et al., 1994). On the first page, rows of the words red, blue, and green appeared in varying order. The subject's task was to read all of the words as fast as possible. The second page consisted of rows of colored rectangles (1.25 x .25 inch) printed in the colors red, blue, and green. The subject was instructed to name the color of each rectangle as fast as possible. The third page, the attention interference task, contained the words red, blue, and green printed in colors different from the color of the word. The subject was requested to name the color used to print the word, rather than read the word, as fast as possible. In each condition the subject's score was the time needed to complete each page.
This is a nonverbal task similar to the verbal form, digit span. The examiner turns over a series of colored disks arranged in a line (one side blue, the other side yellow). The starting trial has two disks, blue side up. The examiner turns over the second disk and then the first disk. The subject, who is watching the examiner, turns the disk back in the same way as the examiner did. The length of the series is increased by one. For most subjects in our study, four disks are likely to be the maximum number that subjects can do (the order of turning can be third, the second, then fourth, and then the first). The test stops when four errors occur consecutively.
The recall of words has been shown to load on a successive factor in several studies by Naglieri and Das (1988) and therefore was considered a marker for successive processing. This task consisted of nine single-syllable words that were presented in a series ranging in length from two to nine words. The subject's score was the total of words recalled in correct order. This task has long been used as a measure of successive processing because it clearly fits the linearity requirement of the successive processing paradigm.
In this task the subject is required to say a series of words 10 times fast, as fast as possible. The version used in this study had three items, the first two had two words, and the third one had three words. The three-item time scores were summed to form the subject's total speech rate score. The maximum time allowed for one item was 60 seconds. Missing values were receded into 181.
This task is similar to those used by Das and colleagues (1979) and Naglieri and Das (1988) as a simultaneous marker task. In this task, the subject looked at a geometric design such as a square or triangle for 5 seconds. The design was immediately represented embedded in a more complex figure. The subject was asked to outline the original stimulus. For a response to be scored correct, all lines of the design had to be indicated without any additions or omissions. The subject's score was the total number correct. The requirement that the object be incorporated into memory as a whole so that all the parts of the figure are interrelated makes this task congruent with the simultaneous paradigm.
The matrices task was developed following the work of Naglieri (1985). It was a simultaneous task that involved analogies using a progressive matrix format. The subject is required to choose one of six options that best complete the abstract analogy. This test has been found previously to load on a simultaneous factor (Naglieri & Das, 1988) as has Raven's colored progressive matrices (Das et al., 1979).
In this task, the subject is asked to point to one of the six different pictures that answer a question printed at the bottom of the page. The question, which is also read aloud by the examiner, involves logical-grammatical relationships represented by the pictures. For example, the question could be, "Which picture shows a man behind a boy?" In another example of the task, the subject is asked, "Which picture shows the arrow pointing to the square in the circle?" Six different designs are presented. The test demands simultaneous processing because the subject must organize the three objects, arrow, square, and circle, into a whole to solve the problem. There were 29 items in the test. The subject's score was the total number or correct responses.
Alexander, J. (1997). Cognitive decline and Alzheimer's disease in Down syndrome. Edmonton: Unpublished doctoral dissertation, University of Alberta.
Ashman, A. F. (1985). Problem solving and planning: Two sides of the same coin. In A. F. Ashman & R. Laura (Eds.), The education and training of the mentally retarded (pp. 169-214). New York: Nichols.
Ashman, A. F., & Das, J. P. (1980). Relation between planning and simultaneous-successive processing. Perceptual and Motor Skills, 51, 371-382.
Baddeley, A. D., & Hitch, G. (1974). Working memory. In G. A. Bower (Ed.), The psychology of learning and motivation, (pp. 47-89). New York: Academic Press.
Baltes, P. B., & Lindenberger, U. (1997). Emergence of a powerful connection between sensory and cognitive functions across the adult lifespan: A new window to the study of cognitive aging? Psychology and Aging, 12, 12-21.
Bensen, D. F. (1987). Clinical diagnosis of Alzheimer's disease. In G. G. Glenner & R. J. Wurtman (Eds.), Advancing frontiers in Alzheimer's research (pp. 235-248). Austin, TX: University of Texas Press.
Birren, J. E., & Schaie, K. W. (Eds.). (1977). Handbook of the psychology of aging. New York: Van Nostrand.
Bowen, D. M., Francis, P. T., & Palmer, A. M. (1987). The biochemistry of cortical and subcortical neurons in Alzheimer's disease. In G. G. Glenner & R. J. Wurtman (Eds.), Advancing frontiers in Alzheimer's disease research. Austin, TX: University of Texas Press.
Burack, J. A., Evans, D. E., Klaiman, C., & Iarocci, G. (2001). In L. M. Glidden (Ed.), International review of research in mental retardation, (pp. 299-320). San Diego: Academic Press.
Carlson, M. C., Hasher, L., Connelly, S. L., & Zacks, R. T. (1995). Aging, distraction and the benefits of predictable location. Psychology and Aging, 10, 427-436.
Crocker, A. C. (1988). Dilemmas of the mental retardation clinician. An assignment for the researcher. In F. J. Menolascino & J. A. Stark (Eds.), Preventive and curative intervention in mental retardation (pp. 357-371). Baltimore, MD: P. H. Brookes.
Cutler, N. R. (1985). Alzheimer's disease and Down's syndrome: New insights. Annals of Internal Medicine, 103, 566-578.
Das, J. P. (1972). Patterns of cognitive abilities in normal and retarded children. American Journal of Mental Deficiency, 77, 6-12.
Das, J. P. (1973). Structure of cognitive abilities: Evidence for simultaneous and successive processing. Journal of Educational Psychology, 65, 103-108.
Das, J. P. (1980). Planning: Theoretical considerations and empirical evidence. Psychological Research, 41, 141-151.
Das, J. P. (1984). Cognitive deficits in mental retardation: A process approach. In P. H. Brookes, R. Sperber, & C. McCauley (Eds.), Learning and cognition in the mentally retarded (pp. 115-128). Hillsdale, NJ: Lawrence Erlbaum.
Das, J. P. (1985). Aspects of digit span. American Journal of Mental Deficiency, 89, 627-634.
Das, J. P. (1992). Beyond a unidimensional scale of merit. Intelligence, 16, 137-149.
Das, J. P. (1995). Some thoughts on two aspects of Vygotsky's work. Educational Psychologist, 30(2), 93-97.
Das, J. P. (1992). A better look at intelligence. Current Directions in Psychological Science, 11, 28-32.
Das, J. P., & Bower, A. C. (1971). Orientating responses of mentally retarded and normal subjects to word-signals. British Journal of Psychology, 62, 89-96.
Das, J. P., & Dash, U. N. (1983). Hierarchical factor solution of coding and planning processes: Any new insights? Intelligence, 7, 27-38.
Das, J. P., Divis, B., Alexander, J., Parrila, R. K., & Naglieri, J. A. (1995a). Cognitive decline due to aging among person with Down syndrome. Research in Developmental Disabilities, 16, 461-478.
Das, J. P., Mishra, R. K., Davison, M., & Naglieri, J. A. (1995b). Measurement of dementia in individuals with mental retardation: Comparison based on PPVT and dementia rating scale. The Clinical Neuropsychologist, 9(1), 32-37.
Das, J. P., Kar, B. C., & Parrila, R. K. (1996). Cognitive planning: The psychological basis of intelligent behavior. New Delhi: Sage Publications.
Das, J. P., Kirby, J. R., & Jarman, R. J. (1979). Simultaneous and successive cognitive processes. New York: Academic Press.
Das, J. P., & Mishra, R. K. (1995). Assessment of cognitive decline associated with aging: A comparison of individuals with Down syndrome and other etiologies. Research in Developmental Disabilities, 16, 11-25.
Das, J. P., & Naglieri, J. A. (1992). Assessment of attention, simultaneous-successive coding and planning. In H. C. Haywood & D. Tzuriel (Eds.), Interactive Assessment (pp. 207-232). New York: Springer-Verlag.
Das, J. P., Naglieri, J. A., & Kirby, R. J. (1994). Assessment of cognitive processes. New York: Allyn & Bacon.
Das, J. P. (1994). Luria, A. R. (1902-1977). Encyclopedia of human intelligence (pp. 678-681). New York: MacMillan.
Deary, I. J., MacLennan, W. J., & Starr, J. M. (1998). Is age kinder to the initially more able? Differential aging of verbal ability in the HOPE study. Intelligence, 26(4), 357-376.
Devenny, D. A., Hill, A. L., Patxot, O., Silverman, W. P., & Wisniewski, K. E. (1992). Aging in higher functioning adults with Down's syndrome: An interim report in a longitudinal study. Journal of Intellectual Disability Research, 36, 241-250.
Devenny, D. A., Krinsky-McHale, S. J., Sersen, G., & Silverman, W. P. (2000). Sequence of cognitive decline in dementia in adults with Down's syndrome. Journal of Intellectual Disability Research, 44, 654-665.
Dodd, B. (1975). Recognition and reproduction of words by Down's syndrome and non-Down's syndrome retarded children. American Journal of Mental Deficiency, 80, 306-311.
Dywan, J., Segalowitz, S. J., & Unsal, A. (1992). Speed of information processing, health, and cognitive performance in older adults. Developmental Neuropsychology, 8, 473-490.
Ferretti, R. P., & Cavalier, A. R. (1991). Constancy in the problem solving of persons with mental retardation. In N. W. Bray (Ed.), International review of research in mental retardation (pp. 153-192). San Diego: Academic Press.
Fristoe, N. M., Salthouse, T. A., & Woodard, J. L. (1997). Examination of age-related deficits on the Wisconsin Card Sorting Test. Neuropsychology, 11, 428-436.
Frith, U. (1999). Paradoxes in the definition of dyslexia. Dyslexia, 5, 192-214.
Frith, U., & Frith, C. (2001). The biological basis of social interaction. Current Directions in Psychological Science, 10, 151-155.
Gibson, D. (1978). Age and pattern or intellectual decline among Down syndrome and other mentally retarded adults. International Journal of Rehabilitation Research, 11, 47-55.
Gokcora, N., Atasever, T., Karabacak, N. L, Vural, G., & Gucuyener, K. (1999). Tc-99m HMPAO brain perfusion imaging in young Down's syndrome patients. Brain and Development, 21(2), 107-122.
Hartley, X. (1985). Receptive language processing and ear advantage of Down's syndrome. Journal of Mental Deficiency Research, 29, 197-205.
Hasher, L., & Zachs, R. T. (1988). Working memory, comprehension and aging: A review and a new view. In G. H. Bower (Ed.), The psychology of learning and motivation, (pp. 193-225). San Diego: Academic Press.
Haxby, J. V. (1989). Neuropsychological evaluation of adults with DS: Patterns of selective impairment in non-demented old adults. Journal of Mental Deficiency Research, 33, 193-210.
Heller, T. (1997). Older adults with mental retardation and their families. In N. W. Bray (Ed.), International review of research in mental retardation (pp. 99-136). San Diego: Academic Press.
Hickson, L., & Khemka, I. (1999). Decision making and mental retardation. In L. M. Glidden (Ed.), International review of research in mental retardation (pp. 227-265). San Diego: Academic Press.
Jarrold, C., Baddeley, A. D., & Hewes, A. K. (2000). Verbal short-term memory deficits in Down syndrome: A consequence of problems in rehearsal? Journal of Child Psychiatry, 41, 233-244.
Kao, C. H., Wang, P. Y., Wang, S. J., Chou, K. T., Hsu, C. Y., Lin, W. Y., Liao, S. Q., & Yeh, S. H. (1993). Regional cerebral blood flow of Alzheimer's disease-like pattern in young patients with Down's syndrome detected by 99Tcm-HMPAO brain SPECT. Nuclear Medicine Communications, 14(1), 47-51.
Kaufman, A. S., & Horn, J. L. (1996). Age changes in tests of fluid and crystallized ability for women and men on the Kaufman Adolescent and Adult Intelligence Test (KAIT) at ages 17-94 years. Archives of Clinical Neuropsychology, 11, 97-121.
Kliegl, R., Mayr, U., & Krampe, R. (1994). Time accuracy functions for determining process and person differences: An application to cognitive aging. Cognitive Psychology, 26, 134-164.
Krupski, A. (1977). The role of attention in the reaction time performance of mentally retarded adolescents. American Journal of Mental Deficiency, 82, 79-83.
Lennenberg, E. H. (1967). Biological foundations of language. New York: Wiley.
Li, S. C. (2002). Connecting the many levels and facets of cognitive aging. Current Directions 2002, 11, 38-43.
Lindenberger, U., & Baltes, P. (1994). Intellectual functioning in old and very old age: Cross-sectional results from the Berlin Aging Study. Psychology and Aging, 12, 410-432.
Luria, A. R. (1966a). Higher cortical functions in man. New York: Basic Books.
Luria, A. R. (1966b). Human brain and psychological processes. New York: Harper and Row.
Luria, A. R. (1970). The functional organization of the brain. Scientific American, 222, 66-78.
Luria, A. R. (1973). The working brain. Middlesex, England: Penguin Books Limited.
Luria, A. R. (1974). Language and brain: Towards the basic problems of neurolinguistics. Brain and Language, 1, 1-14.
Luria, A. R. (1980). Higher cortical functions in man (2nd ed.). New York: Basic Books.
Marcell, M. M., & Cohen, S. (1992). Hearing abilities of Down syndrome and other mentally handicapped adolescents. Research in Developmental Disabilities, 13, 533-551.
Maruyama, K., Ikeda, S., & Yanagisawa, N. (1995). Correlative study of the brain CT and clinical features of patients with Down's syndrome in three clinical stages of Alzheimer type dementia. Rinsho Shinkeigaku - Clinical Neurology, 35(7), 775-780.
Mattis, S. (1988). Dementia rating scale professional manual. Odessa, FL: Psychological Assessment Resources, Inc.
McDaniel, W. F., & McLaughlin, T. (2000). Further support for using the dementia rating scale in the assessment of neuro-cognitive functions of individuals with mental retardation. The Clinical Neuropsychologist, 14, 72-75.
Mori, L, & Nakata, H. (1993). A case of Down's syndrome with progressive dementia of Alzheimer's type. Japanese Journal of Nuclear Medicine, 30, 197-201.
Morse, C. K. (1993). Does variability increase with age? An archival study of cognitive measures. Psychology and Aging, 8, 156-164.
Naglieri, J. A. (1985). Matrix analogies test. Expanded form. New York: The Psychological Corporation.
Naglieri, J. A., & Das, J. P. (1987). Construct and criterion-related validity of planning simultaneous and successive cognitive processing tasks. Journal of Psychoeducational Assessment, 4, 353-363.
Naglieri, J. A., & Das, J. P. (1988), Planning-arousal-simultaneous-successive (PASS): A model for assessment. Journal of School Psychology, 26, 35-48.
Naglieri, J. A., & Das, J. P. (1990). Planning, attention, simultaneous and successive (PASS) cognitive processes as a model for intelligence. Journal of Psychoeducational Assessment, 8, 303-337.
Naglieri, J. A., & Das, J. P. (1997). Das-Naglieri cognitive assessment system. Itasca, IL: Riverside Publishing Company.
Nettelbeck, T. (1994). Speediness. In R. J. Sternberg (Ed.), Encyclopedia of human intelligence (pp. 1014-1019). New York; MacMillan.
Park, D. (2000), The basic mechanisms accounting for age-related decline in cognitive function. In D. Park & N. Schwartz (Eds.), Cognitive aging: A primer (pp. 3-22). Philadelphia, PA: Psychology Press.
Park, D., & Schwartz, N. (Eds.). (2000). Cognitive aging: A primer. Philadelphia, PA: Psychology Press.
Pueschel, S. M. (1987). Cognitive and learning processes in children with Down syndrome. Research on Developmental Disabilities, 8, 21-37.
Reisberg, B., Ferris, S. H., de Leon, M. J., & Crook, T. (1984). Age-associated cognitive decline and Alzheimer's disease: Implications for assessment and treatment. In M. Bergener, M. Ermini, & H. B. Stahelin (Eds.), Thresholds in aging (pp. 255-292). London: Academic Press.
Ross, L. E., & Ross, S. M. (1984). Oculomotor functioning and the learning and cognitive processes of the intellectually handicapped. In P. H. Brookes, R. Sperber, & R. C. McCauley (Eds.), Learning and cognition in the mentally retarded (pp. 217-236). Hillsdale, NJ: Lawrence Erlbaum.
Salthouse, T. A. (1994). How many causes are there of aging-related decrements in cognitive functioning? Developmental Review, 14, 413-437.
Salthouse, T. A. (1995). Refining the concept of psychological compensation. In R. A. Dixon & L. Backman (Eds.), Psychological compensation: Managing losses and promoting gains (pp. 21-34). Hillsdale, NJ: Erlbaum.
Sapir, S., & Nitzburg, A. (1973). Children with learning problems (p. 118). New York: Brunner/Mazel.
Schapiro, M. B. (1993). Neuroimaging in adults with Down syndrome. In J. M. Berg, H. Karlinsky, & A. J. Holland (Eds.), Alzheimer's disease, Down syndrome and their relationship (pp. 173-197). New York: Oxford University Press.
Schupf, N. (2001). Epidemiology of dementia in Down's syndrome. In K. Iqbal, S. S. Sisodia, & B. Winblad (Eds.), Alzheimer's disease: Advances in etiology, pathogenesis and therapeutics. New York: Wiley.
Sejnowski, T. J., & Churchland, P. S. (1989). In M. I. Posner (Ed.), Foundations of cognitive science (pp. 301-358). Cambridge, MA: Bradford.
Silverstein, A. B. (1982). Performance of Down syndrome individuals on the Stanford-Binet intelligence scale. American Journal of Mental Deficiency, 86, 548-551.
Silverman, W., & Wisniewski, H. M. (1999). Down syndrome and Alzheimer disease: Variability in individual vulnerability. In J. A. Rondal, D. Ling, J. Perera, & L. Nadel (Eds.), Down syndrome: A review of current knowledge (pp. 178-194). London: Whurr Publishers.
Silverman, W., Zigman, W., Kirn, H., Krinsky-McHale, S., & Wisnieski, H. M. (1998). Aging and dementia among adults with mental retardation and Down syndrome. Topics in Geriatric Rehabilitation, 13, 49-64.
Snart, F., O'Grady, M., & Das, J. P. (1982). Cognitive processing in subgroups of moderately retarded children. American Journal of Mental Deficiency, 86, 465-472.
Sternberg, R. J. (1984). Macrocomponents and microcomponents of intelligence. In P. H. Brookes, P. Sperber, & R. C. McCauley (Eds.), Learning and cognition in the mentally retarded (pp. 89-114). Hillsdale, NJ: Lawrence Erlbaum.
Sternberg, R. J. (1987). Intelligence applied: Understanding and increasing your intellectual skills. San Diego: Harcourt, Brace, Jovanovich.
Varnhagen, C. K., Das, J. P., & Varnhagen, S. (1987). Auditory and visual memory span: Cognitive processes of TMR individuals with Down's syndrome or other etiologies. American Journal of Mental Deficiency, 91, 398-405.
Vitaliano, P., Breen, A., Albert, M., Russo, J., & Prinz, P. (1984). Memory, attention and functional status in community residing Alzheimer type dementia patients and optimally healthy aged. Journal of Gerontology, 39, 58-64.
Vitaliano, P., Russo, J., Breen, A., Vitiello, M. V., & Prinz, P. (1986). Functional decline in the early stages of Alzheimer's disease. Journal of Psychology and Aging, 1, 41-46.
Vygotsky, L. S. (1978). Mind in society. Cambridge, MA: Harvard University Press.
Waltz, J. A., Knowlton, B. J., Holyoak, K. J., Boone, K. B., Mishkin, F. S., de Menezes Santos, M., Thomas, C. R., & Miller, B. L. (1999). A system for relational reasoning in human prefrontal cortex. Psychological Science, 10, 119-125.
Whiting, H. P. A., & Wade, M. G. (Eds.). (1986). Themes in motor development. Boston: Martinus Nijhoff.
Zeaman, D., & House, B. J. (1963). The role of attention in retarded discrimination learning. In N. R. Ellis (Ed.), Handbook of mental deficiency (pp. 159-223). New York: McGraw.
Zigman, W., Shupf, N., Zigman, A., & Silverman, W. (1993). Aging and Alzheimer's disease in people with mental retardation. International Review of Research in Mental Retardation, 9, 41-70.